











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Dengue is a viral infection transmitted from human to human through the bite of the female mosquito Aedes aegypti or Ae. albopictus, present in more than 100 tropical and subtropical countries (Brady et al., 2012). In the last decade there has been a notorious upsurge of the disease burden mainly in Latin America and the Caribbean (Kourí, 2011). In the Americas, an endemic-epidemic pattern has been described with periodic outbreaks every three to five years, with a transition from an epidemic-endemic status to an only endemic one recently (Montoya et al., 2012).
The Aedes mosquitoes live in close relationship with humans and grow mainly in urban or suburban areas where breeding places and hosts are easily available (Lega et al., 2017). The infection can rapidly spread in a community if there are susceptible people, and if there are high densities of the transmitting mosquitoes, therefore the timely control of the latter is considered one of most important actions of prevention (Bhatt et al., 2013). A key factor that has determined its status as a public health problem is its growing geographic dispersion associated with a high morbidity, which creates a heavy economic and health burden in endemic countries. More than half of the world’s population are at risk of dengue infection, with 100 million symptomatic cases reported each year (Brady et al., 2012).
The spatial and temporal distribution of cases and outbreaks of dengue are related to the interplay of physical, socioeconomic, and climatic conditions, particularly in urban zones with high population density (Bhatt et al., 2013; Zellweger et al., 2017). Temperature is a key determinant, since the increase in environmental temperature has been observed to decrease the duration of the extrinsic incubation of dengue virus, and increases the frequency of the mosquitoes’ propensity to bite. Additionally, temperatures in the range of 22 to 32°C are associated with a higher risk of dengue and are considered the lower and upper threshold of the dengue risk (Fan et al., 2015; Peña-García et al., 2017). Likewise, rainfall patterns are also powerful drivers of a high density of mosquitos (Benedum et al., 2018).
Several studies (Teurlai et al., 2015; Phanitchat et al., 2019; Watts et al., 2020) have analyzed the spatial variability of the incidence of dengue and its relationship with climatic and socioeconomic variables. Overall, a consistent correlation has been found between high incidence rates of the disease and high values of air temperature, rainfall, and humidity; however, also an inverse relation between socioeconomic status and incidence of dengue has been observed (Ogashawara et al., 2019).
The increasing use of new methods and tools for spatial analysis, has contributed to improve the understanding of the geographic distribution of dengue and how it is related to the environment. With this in mind, we aim to describe the intraurban spatial distribution of dengue cases, and to ascertain its potential correlation with socioeconomic and climate determinants at the census-tract level in Hermosillo and Ciudad Obregón, two endemic medium-size cities located in northwest Mexico.
Material and methods
In this study, an ecological approach using Geographic Information Systems (GIS) clustering techniques, and spatially disaggregated health data, are used to examine the spatial correlation between the incidence of dengue and sociodemographic and climatic determinants in the cities of Hermosillo and Ciudad Obregón, in the Mexican state of Sonora, at the northwest of the country. Both cities accounted for 61 % of incidents of dengue cases in Sonora for the period between 2007-2017. Hermosillo is the largest and most populated urban city in the state, in the year 2020 had an estimated population of 936,263 inhabitants and had 577 urban census tracts, known as Basic Geostatistical Areas (BGA) (Gobierno de México, 2020). Its average annual temperature is 24.9 oC, ranging from 17.4 - 34.0 ºC (Navarro-Estupiñán et al., 2018). Meanwhile, Ciudad Obregón has an estimated population of 436, 484 inhabitants and 254 urban BGA (Gobierno de México, 2020). It has an average annual temperature of 25.1 o C (17.6 - 33.9ºC). Precipitation depends on the influence of the North American monsoon that generates about 70 % of the rainfall during the July to September period for both cities. In each of the urban areas, since the year 1966 annual pluvial precipitation for Hermosillo is 356 mm and for Ciudad Obregón is 386 mm.
The socioeconomic profile of each BGA, entails small geographical units containing 25-50 urban blocks and averaging 2,500 inhabitants, and was based on the Urban Marginalization Index (UMI) delineated by the National Population Council and Housing, which is widely used in Mexico to categorize socioeconomic status (SES) at aggregate levels (Gobierno de México, 2015). The UMI includes data about familial income, degree of schooling, housing quality, overcrowding, and health care insurance among others; the UMI stratifies the SES of each BGA in five socioeconomic deprivation strata (very low, low, intermediate, high and very high). In both cities, most BGA are concentrated in the strata of intermediate, low, and very low marginalization, for Hermosillo 340 (68 %) and for Ciudad Obregón 156 (73 %) of the BGA correspond to such categories.
All study procedures were approved by the Research Ethics Committee of the Department of Medicine and Health Sciences, University of Sonora. This research only included secondary data analysis and was therefore considered with no risk to humans.
Data sources
To be considered an official incident, a case of dengue must be confirmed by laboratory techniques such as serology (NS1), Enzyme-Linked Immunosorbent Assay (ELISA) for IgG and IgM antibodies, and real-time polymerase chain reaction (RT-PCR), carried out in the Sonora State Laboratory for Public Health (LESP). Each confirmed case was recorded in the Epidemiological Surveillance System for Vector Transmitted Diseases during the period of January 1st, 2007, to December 31st, 2017. Each eligible case was then georeferenced using the addresses registered in such surveillance platform, and linked geographically with its corresponding BGA; all addresses were mapped using Google Earth® including street, number, intersections, and neighborhood and then transferred to a vector file in a GIS. Only cases with a known address were used and this resulted in a loss of 6,343 (6.6 %) confirmed cases that could not be georeferenced.
Climatological data, temporal and spatial analysis of temperature
Pluvial precipitation and temperature data were obtained for both cities from the Mexican National Water Commission and the Mexican Weather Service regional office. We used records from 1966 to 2018 retrieved from the single climate stations located within the city limits. Historically. in both cities 70 % of the precipitation falls during the summer months of July and September. In addition, both cities have experienced an increase in air temperatures in the same period, and an average of about three heat waves per year for Hermosillo and five for Ciudad Obregón (Navarro-Estupiñán et al., 2018).
As a result of the limited number of climate stations within the city limits, many cities like our study sites are unable to create spatial maps of air temperature and rainfall variability. Notwithstanding, the land’s surface temperature (LST) has been measured using remote sensing applications through various satellites with different spatial and temporal resolutions (Tsou et al., 2017; Yang et al., 2017). The satellites measure the radiation coming from the Earth-Ocean-Earth-Atmosphere systems, including the solar radiation reflected and the infrared radiation emitted (Sorek-Hamer et al., 2016). This allows the use of LST as a proxy for air temperature values in locations with no climate stations, and provides a global understanding about climatic conditions favorable for dengue outbreaks. Thus, Landsat 5 and Landsat 8 satellites’ remote sensing images were used to estimate LST. Three thermal bands at a resolution of 30 m were used with images available approximately every 16 days at 11:00 am local time (Navarro-Estupiñán et al., 2020). To calculate LST, Landsat 5 data was used for the 2007-2012 period, and Landsat 8 images for the years 2013-2017. A total of 354 satellite images were downloaded and used to create a map of the historic average of LST spatial distribution for both cities (Figure 1).

Temporal and spatial data analysis
Descriptive statistics were used to compare gender and age group of selected cases, according to SES of their BGA of residency for both cities. Statistical differences were examined through Chi-squared test using the SPSS 23 program; values of p < 0.05 were considered as statistically significant. Given that the population data of each BGA was obtained from the 2010 national population census, and that our dengue incidences were estimated for the 2011-2017 period, we calculated the softened cumulative incidence rate (CIR) of dengue per 10,000 inhabitants, based on the Bayes empirical method with the use of the GeoDa ™ program version 1.14.0, and thus avoiding overestimating the incidence of dengue cases given the heterogeneity of the population size of each BGA.
Statistical and spatial correlations
The global spatial correlation between the dengue CIR and each BGA UMI was evaluated using the Moran I Index, in which a value close to 0 indicates a random pattern, a value of -1 indicates that the data are too dispersed and a value close to 1 indicates that there is a positive spatial correlation. For the local bivariate analysis, the Local Indicators of Spatial Association (LISA) method was used (Celemin, 2009). All the above was conducted using the GeoDa™ program version 1.14.0, where the value of statistical significance was p≤0.05.
To examine the correlation between dengue CIR, UMI, and LST, we set a temperature threshold lower than 30.6 °C as well as a CIR higher than 90.5 cases per 10,000 inhabitants for Hermosillo. A LST threshold lower than 31.4 °C and CIR higher than 37.6 per 10,000 inhabitants were used for Ciudad Obregón. According to previous studies, a temperature threshold located in the 20th percentile indicates an ideal scenario for the development of Aedes mosquitoes (Fan et al., 2015; Peña-García et al., 2017). Furthermore, for the analysis of the spatial local grouping, the Getis-Ord clustering method was used to find statistically significant “hot and cold” spots within the limits of each city. The Gi* is a Z score, with large range of values, where high scoring implies a more intense clustering (hot spots), and negative values mean cold spots (Peeters et al., 2015).
Results
Incidence of dengue
The final study sample comprised 5 921 confirmed dengue cases, 4 924 (83.0 %) corresponded to the city of Hermosillo and 997 (17.0 %) to Ciudad Obregón. No significant differences were observed in the distribution of cases neither by sex nor age strata, although the highest proportion (30.9 %) of cases occurred in subjects aged 30 to 49 years. When dengue cases were stratified by the UMI of each BGA, the highest percentage corresponded to the very low stratum for social marginalization in both cities (Table I). For Hermosillo, 340 BGA accounting for 94 % of the population, showed better welfare but the highest CIR (78.4 per 10 000 inhabitants) of dengue as well. The opposite was observed for Ciudad Obregón, because although 156 BGA accounting for 97 % of its population were classified as less vulnerable, the highest incidence (35.5 per 10,000 inhabitants) corresponded to BGA with a high degree of social marginalization (Table II).
Tabla 1 Características sociodemográficas de los sujetos de estudio, por sitio de residencia.
| Variable | N (%) | P# | ||
|---|---|---|---|---|
| Hermosillo | Ciudad Obregón | Total | ||
| Sex | ||||
| Male | 2,077 (42.2) | 422 (42.3) | 2,499 (42.2) | 0.932 |
| Female | 2847 (57.8) | 575 (57.7) | 3,422 (57.8) | |
| Age group (years) | ||||
| <10 | 331 (6.7) | 113 (11.3) | 444 (7.5) | 0.000* |
| 10 -19 | 995 (20.2) | 234 (23.4) | 1,229 (20.7) | |
| 20 to 29 | 995 (20.2) | 224 (22.5) | 1,219 (20.6) | |
| 30 to 49 | 1,559 (31.7) | 272 (27.4) | 1,831 (30.9) | |
| 50 to 59 | 578 (11.7) | 83 (8.3) | 661 (11.2) | |
| 60 and over | 466 (9.5) | 71 (7.1) | 537 (9.1) | |
| BGA degree of social marginalization & | ||||
| Very High | 29 (0.6) | 2 (0.2) | 31 (0.5) | 0.246 |
| High | 126 (2.6) | 22 (2.2) | 148 (2.5) | |
| Intermediate | 1,199 (24.4) | 226 (22.7) | 1,425 (24.1) | |
| Low | 1,614 (32.8) | 323 (32.4) | 1,937 (32.7) | |
| Very Low | 1,956 (39.7) | 424 (42.5) | 2,380 (40.2) | |
#Based on a chi square test *Statistically significant at 95 % confidence level.
& Basic Geostatistical Area-level of social marginalization is based on the Urban Marginalization Index from the National Council of Population and Housing.
Table 2 Dengue incidence by degree of social marginalization at the Basic Geostatistical Area-level in the study cities.
Tabla 2 Incidencia de dengue por grado de marginación social a nivel de Área Geoestadística Básica en las ciudades de estudio.
| Marginalization stratum | Hermosillo | Ciudad Obregón | ||
|---|---|---|---|---|
| Incidence* | IQR | Incidence* | IQR | |
| Very High (n = 10) | 42.8 | 26.8-50.4 | 31.2 | 30.0-32.2 |
| High (n = 18) | 53.2 | 33.2-68.9 | 35.5 | 26.9-44.1 |
| Intermediate (n = 92) | 65.9 | 36.0-85.7 | 32.6 | 28.8-37.1 |
| Low (n = 118) | 78.4 | 40.4-93.0 | 34.6 | 27.6-38.6 |
| Very Low (n = 209) | 62.7 | 31.2-78.4 | 31.7 | 28.5-34.1 |
*Smoothed cumulative incidence rate per 10 000 habitants.
IQR=Interquartile Range.
Density of dengue cases per km2
The distribution of cases in Hermosillo was spread-out across the entire city, albeit the largest volume occurred in the north side, ranging between 220 and 273 cases per km2. Similarly, in Ciudad Obregón, the dengue cases were distributed throughout the city, but the density per km2 showed small areas of concentration, discretely more evident in the central and southern areas of the city, with a density per km2 between 77 and 96 cases (Figure 2).

Incidence of dengue cases per 10,000 inhabitants
The highest smoothed CIR found in Hermosillo was 310 per 10 000, while for Ciudad Obregón was considerably lower (62 per 10,000 inhabitants). The higher dengue CIR corresponded to BGA located in the northeast and downtown in Hermosillo (Figure 3a), meanwhile for Ciudad Obregón the higher CIR values were dispersedly pinpointed across the city as shown in Figure 3b.

Spatial correlations and clustering
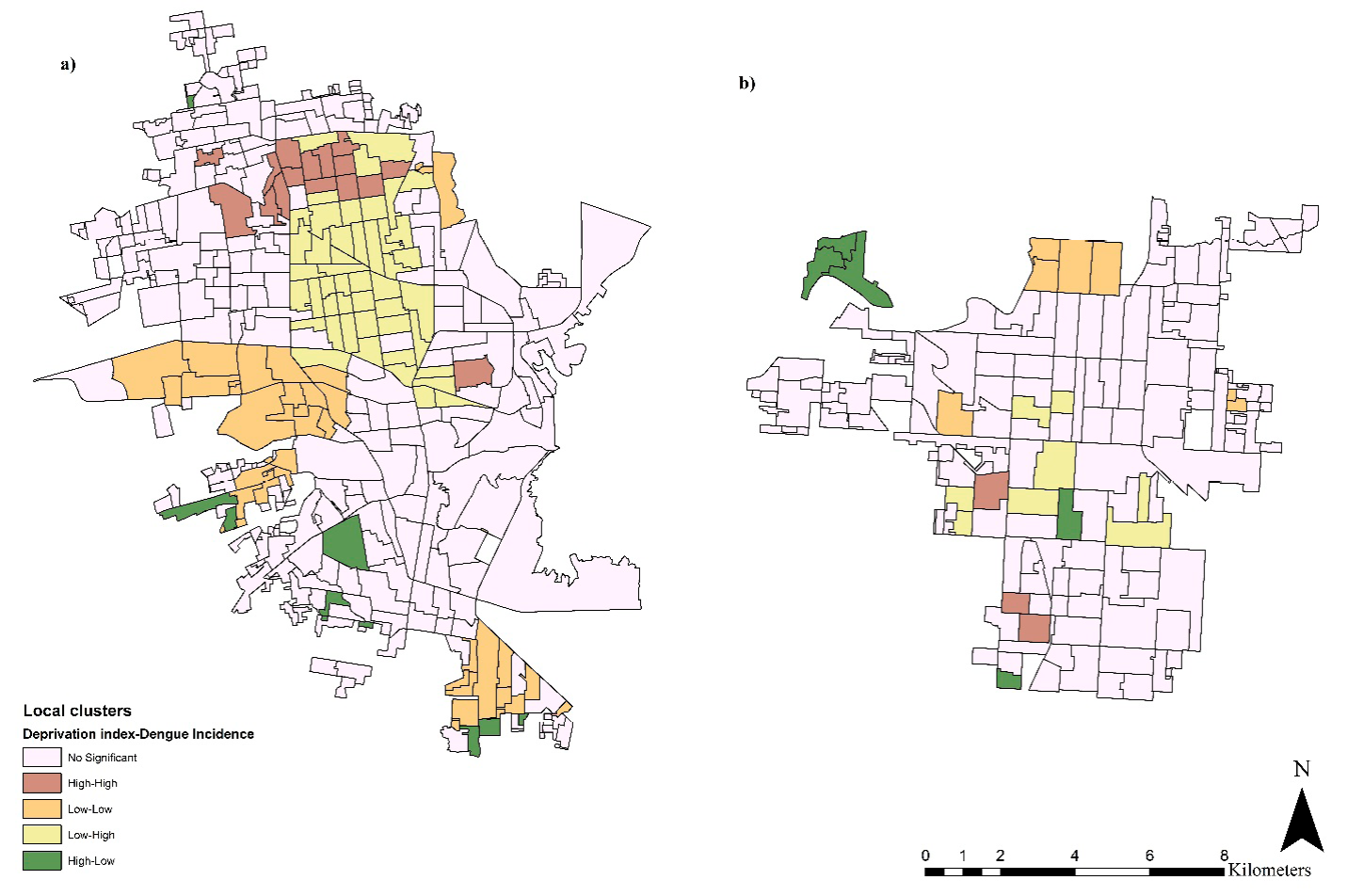
When assessing the global spatial autocorrelation in the city of Hermosillo between dengue CIR and the UMI of each BGA, we did not observe a significant value for the Moran’s Index (I= -0.040). However, when we used the LISA method, a significant spatial autocorrelation was found in BGA with a high incidence of dengue cases and high degree of social marginalization, particularly in the northern parts of the city. Likewise, in Ciudad Obregón the Moran’s I was 0.033, meaning that there is no significant autocorrelation at the global scale. However, the local bivariate analysis showed three areas with a high incidence and a high UMI (Figures 4a and 4b).
Finally, by using the Getis-Ord statistic we found a significant (p <0.01) spatial correlation between the dengue CIR, with the UMI and LST, identifying an area of high risk (“hot spot”) clearly defined, and delimited in both cities. For Hermosillo, the hot spots were located at the central and northern side, where we observed a correlation between an incidence of dengue > 90.5 cases per 10,000 inhabitants, an LST below 30.6 °C, and BGA with high degree of social marginalization. Meanwhile, in Ciudad Obregón three hot spots with statistical significance were found, they were located at the northwest, northeast and southwest sectors of the city; in these “hot spots” a high incidence of dengue coincides > 37.6 per 10,000 inhabitants, a temperature of the land surface lower than 31.4 °C and BGA with high social marginalization as shown in Figure 5.

Discussion
Overall, our findings in the two dengue endemic cities with the largest population in Sonora, Mexico, indicate that although there is no global spatial correlation between the incidence rate of the disease and contextual socioeconomic conditions, there is a local significant correlation at the census-tract level between occurrence of incident cases of dengue and socioeconomic characteristics of the physical space. It drew attention that BGA with medium, low, and very low social marginalization presented the highest dengue incidence, which is consistent with previous research showing a similar pattern of the disease in urban settings (Fuentes-Vallejo, 2017).
The lack of linear correlation between dengue incidence and socioeconomic conditions of peripheral spaces in both cities, can be explained by the fact that more than 90 % of population resides in BGA considered as medium to very low degree of social marginalization. In spite of that, the LISA analysis showed areas of local clusters in such neighborhoods that coincided with a high incidence of dengue with difficulties connecting to the health network, high poverty rates, and other indicators of social vulnerability, which has also been documented in previous Latin-American studies (Mena et al., 2011; do Carmo et al., 2020). Thus, a potential ecological fallacy derived from inaccuracies when measuring socioeconomic attributes of the physical space at the census-tract level, may flaw our findings. To overcome this problem, a smaller scale such as blocks of socioeconomic indicators can be approached, or a more specific classification for cities in the north part of the country that have dengue cases but where the social vulnerability categories appear lower when compared to other localities in the south of the country.
Several social determinants of health are consistently related with the incidence of dengue, such as unplanned urbanization, urban slums, overcrowding, and shortage of running water, sewage, and waste management systems, fostering local transmission of the dengue virus in urban scenarios (Kikuti et al., 2015; Teurlai et al., 2015; Watts et al., 2020; Kolimenakis et al., 2021). Our results are consistent with previous Mexican studies, as we observed a negative relationship between higher incidence rates of dengue and less social welfare at the aggregate level, indicating that better socioeconomic collective development would mitigate the occurrence of the disease in urban areas with limited resources (Escobar-Mesa y Gómez-Dantés, 2015; Reyes-Castro et al., 2017a).
Our results also showed local clusters in BGAs with high dengue incidence rates but low degree of social marginalization, which could be potentially explained by other social variables not included in this study (e.g., population density), as well as climatic conditions of the physical space. In our study, by integrating socioeconomic variables and incidence rates of dengue into a single map, we assess correlations between LST (physical environment) and UMI (social context) finding statistically significant hotspots where a high incidence of the disease coincided with a high surface temperature of the soil, and a high degree of social marginalization. Our findings showed intraurban heterogeneity and overlap with the spatial distribution of infant mortality (Alvarez et al., 2009) and tuberculosis (Alvarez et al., 2010) previously examined at the census-tract level in Hermosillo, and are consistent with recent scientific evidence depicting a similar spatial clustering of arboviral diseases in nine cities located in southern Mexico (Dzul-Manzanilla et al., 2021). Nonetheless, the incidence heterogeneity of dengue that we observed could be explained by a differential in the mosquito density and its spatial distribution as well. It is accepted that heterogeneity in entomological indices (i.e., Breteau index) are related with differential risk of dengue incidence, with higher dengue cases in areas with higher density of mosquitoes, regardless the implementation of control strategies (Peña-García et al., 2016). Entomological data from systematic surveillance should be routinely integrated when assessing spatial distribution of dengue cases.
In addition to contextual social marginalization, individual determinants of welfare such as lower educational level, low family income, among others, contribute to the use of fewer protective barriers (e.g., use of repellants, lack of insecticide pavilions) against the transmitting mosquito. Traditional interventions (e.g., application of larvicides, spatial fumigation) have been found to be less effective in these populations (Reyes-Castro et al., 2017b), and may contribute to the weakening of interventions to prevent and control the transmitting mosquito Aedes at the neighborhood level. Simultaneous statistical modeling of individual and contextual variables, both biological (i.e., fluctuations in dengue incidence and mosquitoes density) and socioeconomic, such as that used in the multilevel analysis, can help to improve our understanding about the interaction of multiple determinants of the social and physical space on the individual risk of dengue, moreover considering the changes in the variance of dengue cases, within and between groups and over time (Diez-Roux et al., 2005; Ordóñez-Sierra et al., 2021).
Despite the consistency and reproducibility of findings from different studies to analyze the spatial pattern of dengue as well as other health events, the clustering techniques are mainly based in registered cases, while socioeconomic and climatic variables used in previous studies were analyzed separately. The combination of different techniques from the spatial analysis are urgent in local contexts similar to ours, not only to search for scientific answers but to be implemented for policymakers and health personnel dealing with intraurban growth of Aedes-borne diseases. Recognition about the applicability of different spatial analysis tools for dengue risk stratification and the design of interventions to prevent and control of mosquito populations, must be accompanied by substantive improvements in the quality of the secondary data sources used routinely in the national health systems, mainly those for epidemiological reports and entomological monitoring.
In this sense, our research has limitations already pointed out in similar Mexican studies (Dzul-Manzanilla et al., 2021; Cortés-Escamilla et al., 2022). Our analyses were based in registered confirmed cases, which may flaw identifying additional hotspots in local areas with less access to health care interventions for the timely diagnosis of the disease. We also had limited data to characterize the effect of urban heat islands and their associated dangers, mostly because air temperature data on land depend on the number of climatic stations and these are missing in many cities across the country (Navarro-Estupiñán et al., 2020). Because we used a Bayesian approach to calculate the cumulative incidence of dengue at the census-tract level, our estimate may be biased impeding to carry out inferences about population dynamics, so new research needs to consider additional information about the implicit conditions involved in dengue transmission such as geometric projections of population and mosquito density. Other limitation of our study is the use of satellite images, which prevented to accurately measure the moments of mosquito heavier activity throughout the day. Future research on this topic can use historical climate datasets freely available in some internet sites (www.worldclim.org).
Conclusions
We found that at the census-tract level disadvantaged populations suffer a higher burden of dengue when compared to areas with better socioeconomic conditions. Although in the study sites the disease does not show a global spatial correlation, and there is a heterogeneous pattern throughout both cities, conditions of high social marginalization and a terrestrial temperature below 31 °C were positively correlated with a higher incidence of dengue at the census-tract level.
The use of spatial clustering analysis methods and tools can be useful to characterize the distribution of dengue cases in small areas in endemic localities. Its practicality and low-cost application can help to detect high-risk areas of dengue and thus plan cost-effective strategies aimed to protect vulnerable populations.

