











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Amyotrophic lateral sclerosis (ALS) is a progressive and fatal neurodegenerative disease that has a worldwide incidence of 0.6-3.3 cases per 100,000 inhabitants. It is characterized by the death of the upper motor neurons located in the motor cortex and lower motor neurons (LMN) located in the brainstem and spinal cord1-5. The degeneration of the corticospinal axons causes thinning and scarring (sclerosis) of the lateral columns of the spinal cord and as the brainstem and spinal motor neurons die a thinning of the ventral roots and a denervational atrophy (amyotrophy) of the muscles of the tongue, oropharynx and extremities occurs, originating muscular rigidity, and spasticity; when LMN are affected, initially, they show excessive electrical irritability, producing spontaneous muscle spasms (fasciculations) but as they degenerate, they lose synaptic connectivity with their muscles causing the consequent atrophy5.
Symptoms usually begin insidiously with the involvement of a specific group of muscles, and then they progressively generalize, it should be noted that the function of the neurons of the oculomotor nuclei and Onuf’s nucleus is usually preserved until the end of the disease1-5, in approximately one-third of the cases the manifestations begin in the bulbar muscles and < 3% of the cases start directly with respiratory muscle weakness (presenting as an unexplained hypercapnic respiratory failure)1,2,6.
In Mexico, there are few data about this condition, a retrospective longitudinal study estimated a presence between 5000 and 7000 cases and described Mexican patients as usually male (male:female ratio of 1.8:1), mean age of onset 47.5 ± 10.5 years, with spinal involvement in 66% of the cases and bulbar affection in 34%, the overall average survival from the onset of symptoms was 68.6 months and 57.8 months since the diagnosis; 3.3% of the cases were classified as family related3,7.
The evolution of ALS to respiratory failure is inevitable and its treatment is mainly aimed to improve symptoms and minimizing the two main pulmonary complications: (1) alveolar hypoventilation (hypercapnic respiratory failure) and (2) poor management of bronchial secretions1; the objectives of the following review are to describe these complications, to propose diagnostic/monitoring guidelines, and to expose the therapeutic options available for the respiratory complications of ALS.
Effects of ALS on respiratory muscles
The physiological consequences of ALS on the respiratory system are directly secondary to the weakness of the respiratory muscles, which can be divided as follows:
– Muscles of inspiration: the muscles involved in inspiration are the diaphragm, sternocleidomastoid, scalenes, and external intercostals4, they generate the ventilation and its weakness, especially that of the diaphragm, leads to a decrease in tidal volume (amount of air entering the lung in each breath with normal effort)8; as the muscle weakness progresses, patients develop a restrictive respiratory pattern with progressive reduction of pulmonary ventilation until it ends in alveolar hypoventilation and subsequent hypercapnic respiratory failure4,9; these alterations manifest as dyspnea, fatigue, orthopnea, night/morning headache, nighttime choking, use of accessory muscles of breathing, and paradoxical breathing when adopting the supine position9-12.
– Muscles of expiration: the main expiratory muscles are the rectus abdominis, internal and external abdominal obliques, the transverse abdominal and the internal intercostal muscles; the decrease in the strength of these muscles generates an ineffective cough with the consequent retention of pulmonary secretions and recurrent infections4,8.
– Bulbar muscles: bulbar muscular weakness, which involves the facial, oropharyngeal, and laryngeal muscles; may affect the ability to speak, swallow, protect the lower airway, and eliminate bronchial secretions; its alteration leads to an ineffective cough, poor handling of secretions, increases the risk of aspiration and makes less tolerable the use of a non-invasive mechanical ventilation device (NIMV), vide infra; the most important symptoms secondary to this alteration are: laryngospasm, sialorrhea, dysphagia, and dysarthria8.
Evaluation of the pulmonary function in patients with ALS
Periodic assessment of respiratory function is imperative to detect early respiratory complications of ALS; these evaluations should be performed at the time of diagnosis and subsequently every 3-6 months, even in the absence of respiratory symptoms4. Respiratory function tests in patients with ALS can be classified as follows:
-
– Direct measurements of muscle strength are those tests that directly measure the strength of the respiratory muscles.
Pleural pressure: it involves the placement of a catheter in the lower third of the esophagus and connect it to a pressure transducer, it is the gold standard for measuring diaphragmatic force; however, little is indicated because of its invasivity9,11.
Maximum inspiratory pressure (MIP): it is a sensitive marker of diaphragmatic weakness in the early stages of ALS and correlates with survival. Normal values almost always exclude inspiratory muscle weakness and pressure lower than −40 cmH2O indicates significant inspiratory muscle weakness. When there is bulbar involvement, patients often cannot perform this procedure correctly due to the inability to form a seal around the mouthpiece (the test is done by placing a focimeter in the mouth and doing a forced inhalation)12.
Sniff nasal inspiratory pressure (SNIP): in this test, the sensor is placed in the nose, which avoids the need to seal the mouth, it is not affected by bulbar weakness which makes it very useful in advanced stages of the disease4, SNIP correlates adequately with transdiaphragmatic pressure. A SNIP < 40 cm H2O correlates with nocturnal hypoxemia13,14, while a SNIP > 70 cm H2O for men and > 60 cm H2O for women excludes diaphragmatic weakness12.
Maximum expiratory pressure: a value < 40 cm H2O suggests expiratory weakness4,12.
-
– Indirect measurements of respiratory muscle strength are those tests that measure lung volumes and flows, which indirectly represents an estimate of the strength of the respiratory muscles, especially the diaphragm:
Spirometry: the most important parameter measured in spirometry for this group of patients is the vital capacity (VC), usually measured through a forced maneuver (forced VC) and more rarely through an unforced or slow expiration (slow VC). Hypercapnic respiratory failure is particularly common with a VC of < 15 ml/kg or an absolute value of 1 L or less12. Most centers consider a reduction of the VC of < 50% as an indication to initiate NIMV; however, the diaphragmatic weakness could be moderate or severe before the VC reaches this point4,9. The ΔVC (VC in the sitting position - VC in the supine position) correlates very well with the diaphragm force measured by transdiaphragmatic pressure (r2 = 0.76, p < 0.001)4 and a 25% drop should be considered at as a sign of compromise the respiratory function10,12. The relationship between VC and muscle strength is not linear, so it is a sensitive marker only in moderate to severe stages of the disease, another limitation of this test is a possible incorrect sealing of the mouth which can alter the measurements12, despite this, repeated VC evaluations are an efficient way to detect respiratory muscle weakness making it a simple, accessible and reliable follow-up test8,13.
Peak cough flow (PCF): it is done with a peak flow meter that is placed in the mouth (requires mouth sealing and is useful when there is bulbar integrity) or through a mask (do not require oral sealing and is used in the presence of bulbar impairment) and the patient is asked to cough heavily on three occasions, taking into account only the highest value, a value < 270 L/min means that the cough is ineffective and indicates the need to implement assistance techniques for cough, while < 160 L/min predicts respiratory failure9,12.
– Gas exchange tests: arterial blood gas analysis is the only gas exchange test useful in patients with ALS and should be performed in all patients; in advanced stages of the disease it is the best indicator of the need for mechanical ventilation when there is a confirmation of a decrease in PaO2 and the elevation of PaCO2 and HCO34,12,14.
-
– Sleep studies: between 17% and 76% of patients with ALS have a respiratory sleep disorder, the most frequent and feared alteration is the sleep-related hipoventilation syndrome; however, it must be considered that patients with bulbar affection have a high risk of obstructive apneas, figure 1. Sleep studies in patients with ALS can be summarized as follows:
– Polysomnography (PSG): it is the gold standard technique for diagnosing sleep disorders of breathing in patients with ALS, the suggested signals to record in this group of patients include: electroencephalogram, electro-oculogram, chin electromyography, snoring, respiratory flow-through two channels (nasal pressure cannula and oronasal thermal sensor), respiratory effort (band in chest and abdomen, ideally inductance plethysmography), electrocardiogram (DII), pulse oximetry, carbon dioxide (can be transcutaneous or exhaled), tibialis anterior electromyography, and body position. Internationally, hypoventilation during sleep is defined when the PSG meets any of the following criteria: (a) an elevation of PCO2 (or a surrogate) > 55 mmHg for 10 min, or (b) an elevation > 10 mmHg of PCO2 (or a surrogate) during sleep, compared to the awake and supine value, up to a value > 50 mmHg for 10 min; this definition is adequate when the study is carried out at sea level15,16, but it must be considered that this definition requires adjustment for moderate altitudes such as Mexico City, table 1. The most reported alteration in sleep architecture among patients with ALS is the decrease in the percentage of rapid eye movement (R) with increased in N1 stage (non-rapid eye movement), which has been associated with decreased survival17,18. The R stage of sleep represents a period of vulnerability for the respiratory mechanics of patients with ALS and is usually the initial moment for the respiratory complications, since muscular atony occurs with loss of the contribution of the respiratory accessory muscles over the tidal volume and the diaphragm is the sole driver of ventilation, this weakness can cause severe alveolar hypoventilation that leads to sustained desaturation and hypercapnia4,8,12,16,17.
– Respiratory polygraph or simplified sleep study: consists of recording only cardiorespiratory variables during sleep, the most used are: respiratory flow, effort, snoring, pulse oximetry, heart rate, and body position, eliminating sleep stages; however, they also do not allow the measurement of CO2, their role in the diagnosis of respiratory disorders of sleep in patients with ALS is limited.
– Nighttime oximetry: it is the most available sleep test, it detects desaturation events; however, it cannot provide information about ventilation and sleep architecture; it has been found abnormal nocturnal oximetry in 40% of patients with ALS without respiratory symptoms, normal respiratory function tests, and normal electrodiagnostic tests of the phrenic nerve and diaphragm18. Nocturnal desaturation correlates with inspiratory muscle weakness and can be used as a guide to initiate NIMV in the absence of PSG; it has been reported that patients who start using NIMV based on nocturnal desaturation can improve their survival4.
– Night capnography: currently, there are capnography devices with transcutaneous measurement, which also incorporate pulse oximetry, which could be useful for diagnosing hypoventilation during sleep, figure 1; however, its diagnostic performance has not been evaluated; at this time, its best indication is as follow-up once the NIMV has been started.
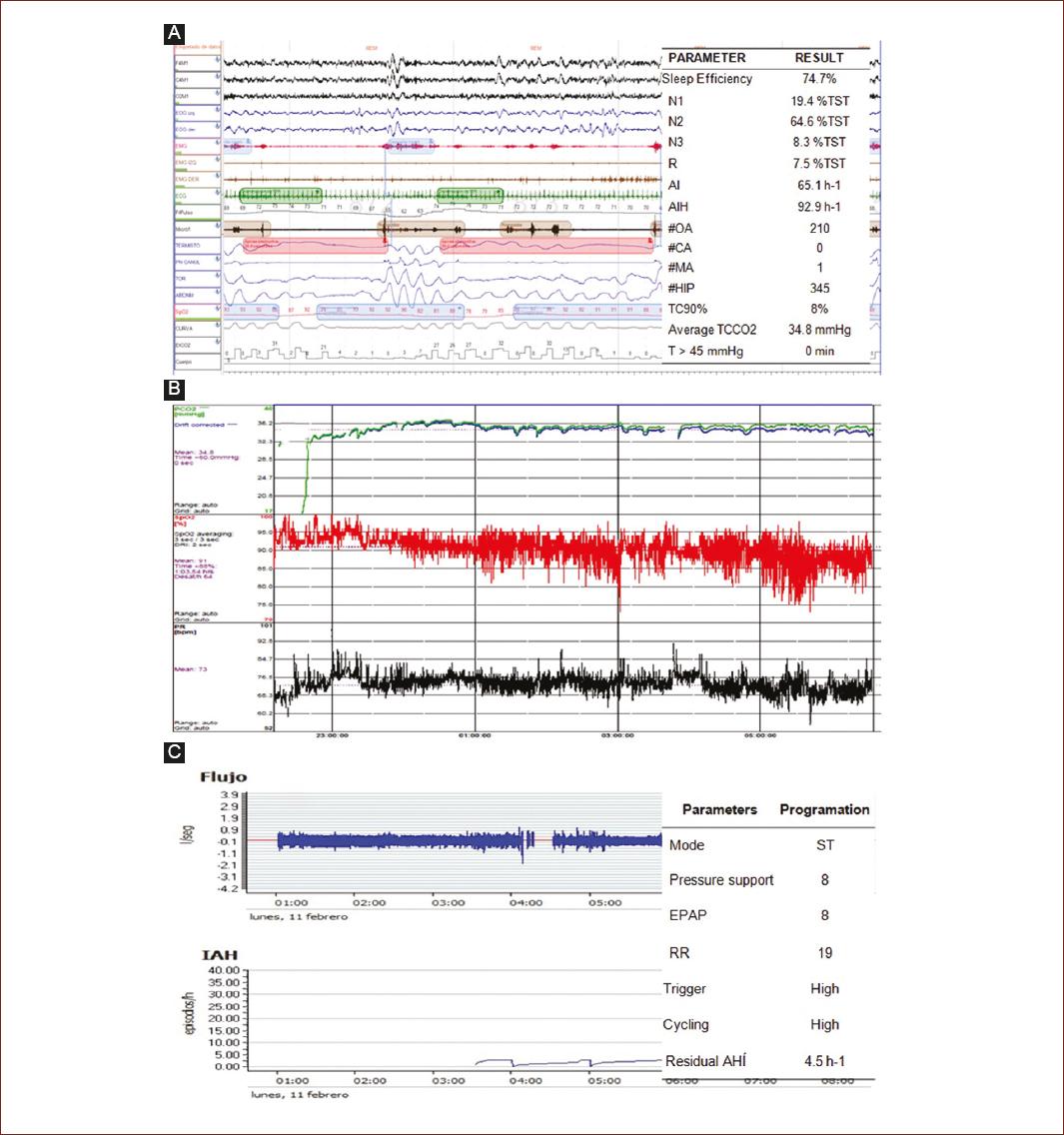
Figure 1 We present the case of a 56-year-old woman diagnosed with ALS with bulbar disease, sent to our service for habitual and intense snoring, witnessed apneas, and excessive daytime sleepiness. The patient presented 26 points on the Bulbar Affectation Scale of Norris, the gasometry in wakefulness was normal and she presented a peak cough flow measured with a mask of 290 L/min. A: Image of polysomnography compacted at 2 min with an increased superficial sleep (N1 and N2), decreased R, and obstructive sleep apneas. B: Transcutaneous capnography obtained during polysomnography, the ventilation during the study was normal. C: Therapeutic test with a bilevel ST positive pressure equipment programmed in the outpatient clinic, a stable flow curve and the optimum residual hypopnea apnea index are observed.AHI: apnea hipopnea index; AI: arousal index; CA: central apneas; HIP: hypopneas; MA: mixed apneas; mmHg: millimeters of mercury; N: no rapid eye movements sleep; OA: obstructive apneas; R: rapid eye movement sleep; RR: respiratory rate; TCCO2: transcutaneous carbon dioxide; TC90%: < 90% saturation time expressed as % of TST; TST: total sleep time; T > 45 mmHg: time in minutes with TCCO2 > 45 mmHg.
Table 1 Definition of hypoventilation during sleep adjusted to moderate altitudes
| A) Elevation of PCO2 (or a surrogate) > 50 mmHg for 10 min |
| B) Elevation > 10 mmHg of PCO2 (or a surrogate) during sleep, compared to the value of awake and supine, up to a value > 45 mmHg for 10 min |
The patient can meet any of the two criteria. mmHg: millimeters of mercury, PCO2: carbon dioxide pressure.
The pulmonary function tests indispensable in patients with ALS are summarized in table 2.
Table 2 Essential pulmonary function tests in the follow-up of patients with ALS
| ALS without bulbar affectation | ALS with bulbar affectation |
|---|---|
| Spirometry + maximum inspiratory pressure | Sniff nasal inspiratory pressure |
| Gasometry | Gasometry |
| Peak cough flow with mouthpiece | Peak flow of cough with mask |
ALS: amyotrophic lateral sclerosis.
Treatment of respiratory complications of ALS
The therapeutic options for modifying the disease are limited; currently, riluzole and edaravone are the only two drugs authorized by the U. S. Federal Drug Administration to reduce deterioration and slow down the progression of ALS19, so, much of the therapy focuses on the management of respiratory complications.
Treatment of alveolar hypoventilation
NIMV
In patients with ALS, respiratory muscle disease with progression to alveolar hypoventilation is unavoidable and cost/benefit its best treatment is NIMV, which prolongs survival and improves symptoms and quality of life20. The best moment to initiate NIMV is when there is hypercapnia (hypoventilation) at night with diurnal eucapnia, so waiting for the onset of daytime hypercapnia to initiate NIMV may be a risk factor to develop acute respiratory failure, but, starting the NIMV in the absence of symptoms or nocturnal hypoventilation may not offer benefits, however, predicting this exact moment of nocturnal hypercapnia with diurnal eucapnia can be difficult, possibly the best way to diagnose it is with serial gasometries and PSGs; however, this may not be accessible, in such a way, the respiratory function tests can be very useful21-23, in the absence of PSG the indications to initiate NIMV in patients with ALS are:
The ventilatory support is usually started at night with the objective that NIMV assumes the work of breathing during sleep12. Inspiratory and expiratory pressures are assessed to maintain a tidal volume of 12-15 ml/kg of ideal weight and an apnea-hypopnea index < at 5/h; this goal becomes increasingly difficult to achieve with the advance of weakness, as the disease progresses, patients will generally begin to extend the use of NIMV during the day and will often progress to a continued use (homecare)4. Factors that adversely affect the tolerability of NIMV are the presence of bulbar symptoms with increased oropharyngeal secretions, cognitive disorders, and claustrophobia13.
A NIMV equipment in patients with ALS can be initiated through two methods:
– With a manual titration through a ventilatory PSG, this implies that trained personnel place a NIMV device and make a manual adjustment of the pressures and respiratory rate, directly evaluating the patient’s respiratory flow and gas exchange, describing the manual titration algorithm of a ventilatory PSG is beyond the scope of this manuscript, If the reader is interested, you can consult the NIMV Mexican Clinical Practice Guideline on Sleep Disorders of Breathing of the National Center for Technological Excellence in Health at the following electronic address: www.cenetec.salud.gob.mx/descargas/gpc/CatalogoMaestro/SS-728-14-Ventilacion_mecanica/GER_VMNI.pdf.
– Or, through an ambulatory clinical ventilation in the office, in this case, the NIMV equipment is programmed with initial parameters already standardized and their effect in the medium and long term is evaluated; in experienced personnel, this method is as good as a manual titration performed with PSG24, the initial clinical settings of a ventilator for patients with ALS are described in table 3, these parameters will depend on the presence of bulbar disease, thus, those with bulbar involvement will require greater expiratory pressure to eliminate obstructive apneas.
Table 3 Programming of equipment for initial NIMV
| Parameter | ALS without bulbar affectation | ALS with bulbar affectation |
|---|---|---|
| Mode | Bilevel ST | Bilevel ST |
| RR (rpm) | 14 a 20 | 14 a 20 |
| EPAP o PEEP (cmH2O) | 4 a 6 | 6 a 8 |
| PS (cmH2O) | 6 a 8 | 6 a 8 |
| Tigger | High or very high | High or very high |
| Cycling | Medium or high | Medium or high |
ALS: amyotrophic lateral sclerosis; EPAP: expiratory positive airway pressure; PEEP: positive end expiratory pressure (synonymous with EPAP); PS: pressure support; RR: respiratory rate; ST: spontaneous/time; NIMV: non-invasive mechanical ventilation.
At the end, patients will need continuous ventilatory assistance (homecare). Once the progressive bulbar weakness prevents the ability of patients to eliminate their secretions (even with mechanical assistance), NIMV is no longer a viable treatment option, so the decision should be made to proceed with the tracheostomy or concentrate in palliation4.
IMV and care at the end of life
IMV through a tracheotomy is an option in specific circumstances:
– When NIMV is not able to maintain adequate ventilation due to the progression of the disease.
– If the use of NIMV is required during most of the day and night (> 16 h/day).
– Bulbar muscular deterioration that does not allow a tolerance of NIMV, with a deficient control and elimination of secretions that are not improved by pharmacological strategies and mechanically assisted coughing techniques.
IMV is strongly associated with prolonged survival in ALS; however, an improvement in quality of life is less clear, patients with tracheotomy continue to experience progression of the disease, so some patients eventually progress to a state without communication or movement4.
It is important that patients and family members recognize that the care required by patients with IMV at home is complex, at least two highly trained and motivated family members are needed for special care of the stoma, hygiene of the cannula, and correct aspiration technique of secretions; therefore, the IMV in these patients causes an increase in the cost of treatment, with significant emotional and social impact on both the patient and their caregivers, and can reduce the quality of life of both4.8.
Given that the ALS has a predictable course, it is important to discuss with the patients and caregivers the possible invasive and non-invasive management options as soon as possible, with the aim of avoiding these decisions in the context of an abrupt clinical deterioration and giving them, patients and relatives, the time to reflect; the decision to perform a tracheotomy should only be taken with the informed consent of the patient and after a careful discussion about its pros and cons4.8,23.
Diaphragmatic pacemaker
The use of diaphragmatic pacemakers has been investigated as a way to reduce the decline in lung function; however, randomized studies reported an increase in mortality, which is why they do not represent a treatment option for respiratory failure in patients with ALS4,13,23.
Management of bronchial secretions in patients with ALS
An essential mechanism of protection of the airway is the ability to cough when the clearance of bronchial secretions is impaired; this represents a serious threat to life25. Effective cough initially requires full inspiration, followed by a glottal closure and by last an intense contraction of the expiratory muscles to generate adequate pressures and flows to move the bronchial secretions8, these phases can be affected in different ways and in different magnitudes in all the neuromuscular diseases; however, in ALS the affliction at three phases are progressive and severe; thus, the diaphragmatic weakness will decrease the initial inspiration (this is the condition that takes longer to appear), the bulbar alteration will deteriorate the glottic closure and the weakness of the rectus abdominis, obliques, and internal intercostals will wear out the expiratory phase (it is usually the initial alteration)25. Physical therapy such as percussion or other techniques to mobilize secretions is not enough in patients with ALS12. Cough assistance techniques are indicated when patients’ PCF falls below 270 L/min; these techniques can be classified as follows:
– Manually assisted cough: manual cough should be considered in patients with conserved glottic function, since artificial inspiratory flows and assisted abdominal movements replace the respiratory muscles, but nothing can replace glottic function8,12,13; this technique is carried out in a simple way following this steps:
• With a bag-valve-mask ventilation device (Ambu©) several assisted breaths are made, asking the patient to retain the air in each of them with the objective of expanding the lung close to total lung capacity (the maximum amount of air inside the thorax after a forced inspiration)12,13,26,27.
• Then, the patient will cough but will use an abdominal push to increase the intra-abdominal pressure and exhale forcefully; this push can be exercised by an assistant directly with their hands on the abdomen of the patient12.
• It is common for bronchial secretions to remain in the pharynx or mouth from where they will have to be extracted with a vacuum.
– Mechanical techniques: mechanically assisted cough or mechanical insufflation-exsufflation (MIE) is the most effective alternative in these patients to avoid the accumulation of bronchial secretions, it is especially indicated when the PCF is < 160 L/min23,25,26, is performed with a mechanical device that accumulates several breaths with positive pressure before suddenly changing to a negative pressure:
• An oronasal mask or tracheotomy connector is placed and positive pressure is applied; the applied pressure can vary between +20 and +40 cmH2O.
• To simulate a normal cough, the pressure is suddenly changed to negative values, the pressure generated in this phase can vary between –20 and –40 cm H2O28.
• Some MIE equipment incorporates oscillatory waves to fluidize secretions29.
• It is common for the bronchial secretions to remain in the pharynx or mouth from where they will have to be extracted with a vacuum.
• 6-8 MIE cycles per session should be administered27.
Assisted coughing techniques should be applied at least 3 times a day or more frequently as needed4,26.
Isolated symptoms and special situations
Sialorrhea
Sialorrhea among patients with ALS is common, can be socially disabling and hinder the use of NIMV13; it can be treated with oral suction or with pharmacological measures through medications with mild antimuscarinic effect such as oral glycopyrrolate (2-8 mg/day), amitriptyline (75-150 mg/day), and transdermal scopolamine patch (1.5-3 mg/72 h) among others; if an acceptable therapeutic effect is not obtained, injection of botulinum toxin into the salivary glands can be used; however, as the toxin can spread to nearby muscles, it can worsen dysphagia and should be reserved only for gastrostomy patients; another option to consider is the use of local radiotherapy, which has fewer side effects, but does not last as long as botulinum toxin10,13,30.
Dyspnea
Although there are no clinical trials of the management of dyspnea in ALS, the recommendations for the control of it arise from the clinical contexts where dyspnea is a characteristic symptom of the disease in its terminal phases and is an integral part of management in palliative care31. For distressing dyspnea, first-line drugs are systemic opioids, which can be indicated from the onset of the symptom and not only in the final stage of the disease32. Treatment begins with an initial dose equivalent to 2.5 mg of morphine sulfate every 4 h. The dose should be increased by 30% every 12 h until dyspnea improves or intolerable side effects develop. When an adequate relief of symptoms is obtained, the use of a long-acting opiate such as oral or transdermal fentanyl is recommended. For exacerbations of dyspnea, doses of recap are used, which are 10% of the total daily dose administered as needed each hour for oral medications or every 30 min for parenteral medications.
Vaccination
Vaccination against influenza and pneumococcus is recommended following the corresponding schemes4.
Oxygen
Patients with early respiratory failure should not be treated with oxygen without other forms of ventilatory support (NIMV or IMV), since oxygen therapy in respiratory failure suppresses the hypoxic drive and increases the risk of hypercapnia13.
Acute respiratory failure
Despite the lack of randomized controlled studies, there is agreement on the effectiveness of NIMV to prevent endotracheal intubation in acute respiratory failure events, thus, in one study, three out of four patients who had previously rejected the tracheotomy, but not the NIMV they survived an episode of acute respiratory failure treated with NIMV; the factors associated with success are the correct programming of the ventilation devices, the availability of several types of interfaces (masks) and the proper management of secretions8; the main factor limiting the success of NIMV during a respiratory infection is the severity of bulbar dysfunction with a cutoff point on the Norris Scale of 12 points (sensitivity 0.90, specificity 0.92, positive predictive value 0.76, and negative predictive value 0.97)33.
The complete pulmonary complications of ALS and their treatments are summarized in table 4.
Table 4 Respiratory complications of ALS and their treatment
| Alveolar hypoventilation | Poor management of bronchial secretions | ||
|---|---|---|---|
| Pathology | Treatment | Pathology | Treatment |
| Sleep-related hypoventilation syndrome | Nocturnal NIMV | Pneumonia | –Hospital management –Antibiotic –Techniques of assisted cough |
| Chronic respiratory failure | –Home care (24 h of MV) –Tracheotomy |
V/Q alterations | Techniques of assisted cough |
| Acute respiratory failure | Emergency management/ICU | Sialorrhea | –Amitriptyline –Scopolamine –Botulinum toxin |
| Dyspnea | –Opioids –NIMV |
Fail to NIMV | –Tracheotomy –Palliative care |
ALS: amyotrophic lateral sclerosis; ICU: intensive care unit; MV: mechanical ventilation; NIMV: non-invasive mechanical ventilation; V/Q: ventilation/perfusion.
Follow-up
The care of patients with ALS should be multidisciplinary and ideally should be performed in specialized centers involving: neurologists, pulmonologists, otolaryngologists, rehabilitation physicians, psychologists, and psychiatrists among others; all with the common goal of increasing survival, improve quality of life, and decreasing hospitalizations from acute events; these specialized centers usually offer appointments with different specialists in a single visit, reducing the trips of patients to the hospital and, consequently, their fatigue. Quarterly appointments are usually proposed, with variations according to the progression of the disease13.
Conclusions
The respiratory complications of ALS represent a serious problem for people with this disease and are secondary to the weakness of the muscles that generate respiration; non-IMV and assisted cough (manual or mechanical) are the two most cost/effective techniques to treat alveolar hypoventilation and poor secretion management, respectively, these tools used in conjunction prolong survival and improve the quality of life of the patients with ALS.

