











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Understanding OB requires the development of models that facilitate the analysis, prognosis, and recognition of its behavior, all which enables us to address it (WHO, 2005). One proposal for model generation used in Artificial Intelligence (AI) is the Perceptron Model of Artificial Neural Networks (ANN). It has proved to be useful for a broad understanding of the factors that influence the relationship between the input, the hidden layers (synapsis) and the output or dependent variables. Multilayer perceptron (MLP) is a nonlinear interaction model of the relationship between variables with a high level of connectivity. Backpropagation allows for networks to learn based on least squares error correction, and its main objective is that the networks learn to identify patterns and generate categories of information (García & Espinosa, 2013). This process is as follows: among n cases, the ANN algorithm randomly chooses some and excludes others until it finds, depending on the number of trials, the model that best fits the input and output variables. In this way, the use of the results of ANN models enables health professionals to make more specific and effective decisions for interventions; influencing well-being and life quality of patients (Bajo & Ballesteros, 2002; Arias et al. 2019; Sarmiento-Ramos, 2020).
From a neuropsychological perspective, there is a growing interest to understand the neural functions and substrates of complex cognitive processes related to OB, particularly executive functions (EF), which are supported in planning, self-monitoring, inhibition, and decision making performed daily (Allan et al., 2016; Tirapu et al., 2012).
It has been suggested that obese individuals with a sedentary lifestyle show low results in inhibitory control and working memory tasks, as well as a lower neurocognitive performance (Tsai, 2019) correlative to BFP, which has a negative impact on performance of cognitive control tasks, (Huang et al., 2019; Yang et al., 2018) while in individuals with a healthy weight executive functioning is not impaired (Calvo et al., 2014; Narimani et al., 2019).
OB entails a greater accumulation of body fat and its redistribution into adipose tissue for storage (Carlson, 2014; Brandan et al., 2014). This accumulation results in an energy imbalance which is reflected mainly in weight gain and waist and hip circumference (Carlson, 2014; Cherbuin & Walsh,2019). This is the reason why BFP is a more effective measure at predicting health risks than the simple measurement of gross weight or Body Mass Index (BMI) (Calvo et al., 2014; Huang et al., 2019; Narimani et al., 2019).
The use of ANNs has been helpful in finding the relation between environment and the prevalence of OB. In a study conducted in the USA, AI was used to identify more than 150, 000 satellite images and establish links with OB prevalence and health indicators, such as the level of physical activity of people. The final algorithm found, indeed, a relation between high population density, a high number of expressways, fewer parks and green spaces and high prevalence of OB (Cardozo et al., 2016). Heydari, Ayatollahi & Zare compared ANN and binary logistic regression to identify degree of obesity in a group of adults with different degrees of fat percentage. They found that both models were efficient in identifying the degree of obesity (2012). In another study, Ergün (2009) based on the need to have an automated system for the recognition and monitoring of obesity, also compared a multilayer neural network model against a binary logistic regression model, concluding that the neural network is better than the logistic one.
Therefore, the objective of this study was to identify the synaptic weights of the ANN whose input variables are the executive functions (EF) and health lifestyles as predictors of Body Fat Percentage (BFP) in a group of adult subjects with low, normal, high, and very high body fat levels.
Material and Methods
This was a non-experimental, cross-sectional, explanatory, quantitative with a non-probabilistic design, convenience sampling, n = 40 adults aged between 18-38 years old. All the participants were residents of Azcapotzalco, Miguel Hidalgo and Cuauhtémoc, mayors of Mexico City, and were evaluated from November 2019 to February 2020.
Instruments and Measurements OQ, Overeating Questionnaire
It is a self-administered instrument with a five-point Likert-type scale (Not at all, A little, Moderately, A lot and very much) used to evaluate habits, thoughts and attitudes related to overweight and OB. It contains 80 items that measure cognitions, behavioral cognitions, behaviors-habits, emotions, and attitudes related to obesity. For its construction, it was applied to an n=1,788 North American individuals between the ages of 9 and 98 years old. Two areas were found: one for Inconsistency (INC) and one for Defensiveness (DEF). Eight scales for Habits and Attitudes: Overeating (SOB), Undereating (SUB), Cravings (CRAV) and (SUB), Food cravings (ANT), Expectations with eating (EXP), Rationalizations (RAC), and Motivation to lose weight (MOT). The latter scales assess variables related to general habits and psychosocial functioning: Habits (Hábitos), Eating Habits (HAB), Eating Expectations (EXP) psychosocial functioning: Health Habits (SAL), Body Image (COR), Social Isolation (AIS), and (AIS) and Affective Disturbances (AFE). It has an internal consistency of 0.94 to 0.88, and correlates with BMI scores and with other scales that measure health habits, social functioning and social functioning. The authors report a reliability of 0.82 (Cronbach’s alpha) and construct validity on subscales of Food Cravings and Motivation of 0.26, for Food Cravings and Motivation; 0.68 between Food and Motivation; 0.68 between Social Isolation and Affective Disturbance; Health Habits and Food Intake 0.53 (William and Warren, 2007). In 2014 a factor analysis was conducted which yielded 9 factors, which were: social isolation, stress, body image, depression, health habits, expectations related to eating, overeating, motivation to lose weight and weight concern, all of them integrated in 30 items (Psihas, 2014). The questionnaire had acceptable validity and reliability (≥.76) in the Mexican sample, however the sample was very small compared to the original one, so it was decided to use the latter in the present investigation.
Neuropsychological battery of executive functions and frontal lobes (BANFE -2).
The 15 sub-tests that integrate the battery are divided based on anatomical-functional criteria that evaluate complex functions of the orbitofrontal cortex (OFC), prefrontal cortex (PFC), through the sub-tests: stroop effect, card game and mazes; of the dorsolateral prefrontal cortex (DLPFC) through: self-directed signaling, spatial working memory, alphabetical word sorting, card sorting, maze and Hanoi tower; and of the anterior prefrontal cortex (aPFC) through: semantic classification, choice of sayings and metamemory. The qualification is carried out through the quantitative and qualitative analysis of successes and errors, based on the concept of the functional system postulated by Luria and has normative data for the Mexican population with 450 subjects between 6 and 80 years old with different schooling ranges. (Flores et al., 2014).
This analysis allows to obtain an overall performance index and a performance index of the three pre-frontal areas evaluated, the standardized scores have an average of 100 and a standard deviation of 15. The interpretation of the total score and of each of the areas allows to classify the execution of a person as follows: high normal (116 onwards), normal (85-115) slight to moderate alterations (74-84) and severe alterations (less than 69). It is possible to obtain the standard scores for each of the sub-tests through the performance profile, the standard scores for the sub-tests have an average of 10 and a standard deviation of 3. (Flores et al., 2014). Therefore, subscales were chosen that evaluate inhibitory control, rule following and risk-benefit processing, cognitive processes and emotional regulation, which are related to deregulated behaviors related to fat percentage.
RENPHO ES-24M Smart Body Composition Scale
The RENPHO ES-24M Smart Body Composition scale was used for the measurement of body composition data; it sends a safe low-voltage electrical signal that runs through the body. It allows us to obtain data such as weight, BMI, BFP, and visceral fat level.
BFP Classification and values
Women: Low <21%, Normal 21 - 32.9%, High 33 - 38.9% and Very high> 39% Men: Low <8%, Normal 8.1 - 19.9%, High 20 - 24.9% and Very high> 25% (Cardozo,et al., 2016).
Ethical considerations
This study was carried out following the criteria of the protocol and in accordance with the Ethical Principles for Medical Research Involving Human Subjects, this research had a minimal risk for participants. (AMM, 2013). This research was approved by the CICS-UST Ethics Committee (CEI-CICS-009).
Analysis and mathematical method
We used measures of central tendency, dispersion, percentages, and MLP ANN (Turban et al., 2007) with three feedforward connected layers to identify the hidden layer connected to the output layer. The output variables were the predicting variables among the variables of the stimuli or input layer, which are the BANFE-2 and the OQ scales. For validation, we used 10-fold cross-validation. The learning algorithm used was backpropagation (García & Espinosa, 2013).
Procedure
A call for voluntary participation was made in the Centro Interdisciplinario de Ciencias de la Salud, Unidad Santo Tomás, Instituto Politécnico Nacional. We asked the participants to sign the informed consent and then we measured their BFP using the RENPHO ES-24M Smart Body Composition Scale. Once the data was collected, participants were divided into four groups according to their BFP: Low, Normal, High and Very High. None of the participants was classified in the Low Group.
The instruments were applied collectively at the Centro Interdisciplinario de Ciencias de la Salud, Unidad Santo Tomás, Instituto Politécnico Nacional by the authors.
We developed a MLP ANN whose output variables were BFP and metabolic age; and whose input variables were BANFE-2, OQ and gender. SPSS V 22.0 software was used for this analysis.
Results
The sample was composed of 40 adults of whom 55 % were women (n = 22). The average age was 24.5 years (SD = 3.87). Regarding anthropometric measurements, average BFP was 26.86 (SD =7.23), and average visceral fat was 8.49 (SD =3.92) (Table I).
Table I Means by groups of body fat percentage
| Table I | |||
| Sex | Group | n |
|
| Woman | Normal
High Very high Total |
16
8 3 27 |
23.56 ± 4.55
34.80 ± 1.65 37.66 ± 4.61 28.46 ± 7.15 |
| Man | Normal
High Very high |
6
3 13 |
14.93 ± 1.02
24.80 ± 5.99 29.54 ± 2.54 |
Note: x= average, SD= Standar Deviation.
Table II describes the results of the means and SD. As described in the table, differences in fat percentages are observed, higher in women compared to men.
Table II
| OQ Scales |
|
| Overeating | 58.27 (10.98 |
| Defensiveness | 51.20 (7.75) |
| Undereating | 54.00 (7.25) |
| Craving | 55.80 (7.12) |
| Expectations about eating | 55.49 (8.96) |
| Rationalizations | 54.47 (8.9 |
| Social isolation | 52.92 (11.7) |
| Affectivity | 60.57 (8.58) |
| Motivation | 60.35 (9.59) |
| Healthy habits | 49.45 (10.83) |
| Body image | 53.96 (9.78) |
Note: x= average, SD= Standar Deviation.
Table III shows the applied subtests, which were: Stroop effect, card game and mazes, these tests evaluate the orbitofrontral cortex functions which estimates the ability to detect and avoid risk selections, to exercise inhibitory control, to respect limits and follow rules. For the analysis, the operating index of the orbitofrontral area was obtained based on the standardized scores allowing to group the participants according to the level of alteration of the evaluated cognitive functions.
Table III
| BANFE-2 Scales |
|
| Orbitomedial Performance Score | 81.27 (21.24) |
| Labyrinths | 7.08 (3.713) |
| Percentage of Risk Cards | 9.84 (2.6) |
| Total Card Game | 9.10 (3.38) |
| Stroop A Errors | 7.57 (4.38) |
| Stroop A Time | 9.69 (2.87) |
| Stroop A Successes | 6.33 (4.14) |
| Stroop B Errors | 8.61 (4.23) |
| Stroop B Time | 10.22 (2.17) |
| Stroop B Successes | 8.86 (4.05) |
| Maintenance errors, Classification of cards | 5.22 (3.16) |
Note: x= average, SD= Standar Deviation.
Graph 1 and Graph 2 show the results of average synaptic weights of input factors (OQ and BANFE-2 scales) for BFP output factor (synaptic weight percentage for each input factor).
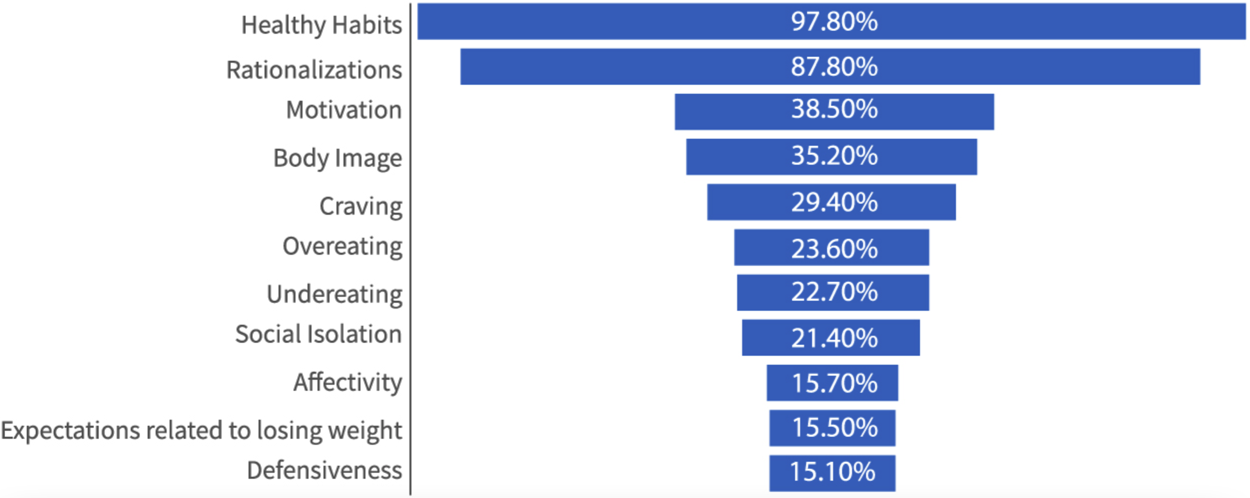
Note: The averages of the neural weights of all the tests run for the OQ are presented. Health habits and Rationalizations for eating, have a high synaptic weight separately; later, Motivation, Body image and Cravings, with average weight.
Graph 1 Average synaptic weight of input factors (OQ).
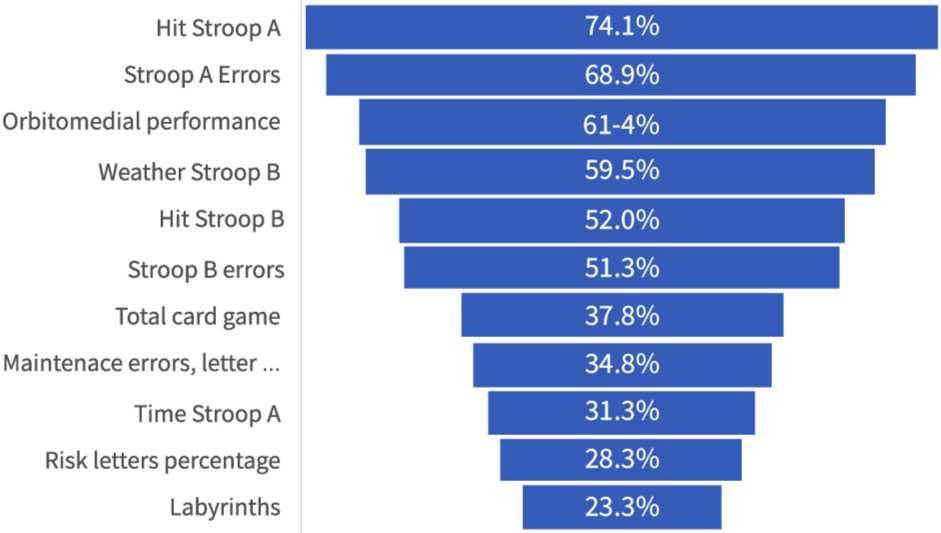
Note: The averages of the neural weights of all the tests run for the BANFE-2 are presented. In this graph we observe a greater distribution in the importance of synapses separately, which goes from Hit Stroop A to Total card game.
Graph 2 Average synaptic weights of input factors (BANFE-2).
The model shows a reduction in the error (see Graph 3) as the tests were run, with a low final error of 0.149 and an average error in the first test of 0.30 for the OQ variables and neuropsychological variables.


On the other hand, the model for BANFE-2 also shows a reduction in error (see lower graph) as the tests were run, with a low final error of 0.18 and an average error in the first test of 0.46. The percentages of synaptic weight of the input factors of OQ scales Healthy Habits, Rationalizations, Motivation and Body Image showed a greater synaptic weight in the ANN, with two input layers for the output factor BFP.
Discussions
The main objective of this research was to identify the synaptic weights of the ANN, whose input variables were the executive functions (EF) and health lifestyles as predictors of Body Fat Percentage (BFP), in a group of adult subjects with low, normal, high, and very high body fat levels.
The implementation of ANN allows predictive models for the estimation of contextual intake variables and neuropsychological variables that contribute interactively to BFP, and that can be generalized for men and women aged between 18-40 years old.
Error correction by least squares allows the learning of patterns of neural networks, with these patterns, categories are generated (García & Espinosa, 2013).
These categories were confirmed with the application of two instruments, one for neuropsychological variables and another for healthy habits of overeating and undereating. We found that Healthy Habits and Rationalizations to Lose Weight, as well as Stroop A Successes, Stroop A Performance, Orbitomedial Performance, Stroop B Time, Stroop B Successes and Stroop B Errors have high synaptic weights for the output variable BFP. Therefore, these models can provide useful tools for the study of complex related variables in the context of OB, in addition to the development of more specific interventions that integrate healthy habits, as confirmed by Adavi, Salehi & Roudbari (2016), and intentional neurological interventions that integrate specially the orbitomedial area. As we can see, the average error decreases in test 10, which allows us to identify in both measurements an adequate adjustment of the ANN (synapse), both for the variables of healthy habits, and for the neuropsychological variables (variables of input) in relation to the percentage of fat (output variable), confirming what was stated by Huang (2019).
As Yang (2018) and Tsai (2019) suggest, Ob and therefore body fat, would generate lower neurocognitive performance mainly in inhibitory control tasks, however our findings transcend this hypothesis, since we found a synaptic weight of the subtest for the orbitofrontal area, related to both executive functions and emotional regulation.
In the multilayer neural network with architecture 9, 3, 3, 1, the specific finding of the synaptic weight of the OQ subscale Rationalizations to Continue Eating to BFP is related to the type of dysfunctional cognitive response of obese individuals, which allows them to disengage from the responsibility of maintaining a healthy body weight.
In the multilayer neural network with architecture 12, 3, 3, 1 with the BANFE-2 input variables and output variable BFP, we found that inhibitory control performance has the highest synaptic weight as the predictor of adiposity. Stroop is related to the processing speed and the ability to control the interference of other brain structures not congruent with a cognitive task, i.e., mechanisms of motor and behavioral inhibition (Golden, 2020; Lubrini et al., 2009 as cited in Blazquez et al. 2009). Therefore, obtaining meaningful data in Stroop A and B Errors and Successes relates to the effectiveness of these mechanisms to control and coordinate simple cognitive processes.
This study shows the relevance of using ANN for simultaneous analysis of neuropsychological and healthy lifestyle data for the investigation of OB prevention and treatment, especially when considering EF performance regarding intake for the evaluation and modulation of hunger, satiation and satiety, craving and emotional changes in its corresponding behavioral response (García-Flores, 2017; Benelam, 2009), as environmental factors have been shown to impact biological processes and body weight.
As Ergün (2009) and Sarmiento-Ramos (2020) reports, the use of ANN allows health professionals to make more precise and effective decisions to improve well-being and quality of life.
Conclusions
Maintenance of Healthy Habits subscale measures the regularity of behaviors considered as good health practices; therefore, such synaptic weight for the BFP would be related to an inability to modify healthy behaviors. The use of nonlinear mathematical models allows to identify open links between the dependent variables, in this case the percentage of fat, with differential weights (synaptic networks), and the independent variables (input variables), in this research neuropsychological factors, habits and cognitions related to overeating and undereating as measured by the OQ. Neural Networks are a novel method that can replace linear regressions or accompany these results, both to compare or even strengthen these findings. The orbitofrontal cortex and the prefrontal area are responsible for processing information and inhibiting responses, as well as habits, reasoning style, image perception and cravings which are factors that are related to the percentage of fat. These findings may redirect behavioral therapeutic goals, seeking greater specificity and effectiveness.
For subsequent research, we suggest expanding the sample in clusters by fat percentage, age groups and sociodemographic factors, and compare with linear regressions or binary logistic regressions.

