











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Osteoporosis is a progressive systemic skeletal disorder characterized by a decrease in bone mass and microarchitectural deterioration of bone tissue leading to bone fragility and increased susceptibility to hip, spine and wrist fractures.1
Atypical fractures are characterized by presenting after a minimal contusion, or in the absence of trauma; with periosteal or endostal localization, in the lateral cortex, complete or incomplete, with transverse tracing and minimal comminution.2 Atypical femoral fractures are associated with the use of bisphosphonates, a rare adverse reaction associated to prolonged treatment with these drugs.3
Case report
A 65 years old female, that on March 13, 2016, mentioned having a fall from her own height. With a medical record of osteoporosis, seven years of diagnosis in treatment with risedronate 35 mg and calcitriol 0.25 μg; systemic arterial hypertension five years of diagnosis, treated with candesartan 8 mg and amlodipine 5 mg; hypercholesterolemia treated with simvastatin 20 mg.
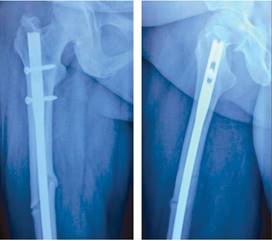
Anteroposterior and lateral radiographic studies of the right femur show a continuity solution at femoral diaphysis with oblique tract, dislodged, without comminution, and cortical thickening. It was treated with CRIF with an antegrade locked intramedullary nailing (Figure 1). She is discharged 48 hours postoperatively with adequate evolution. Upon discharge, she is treated with teriparatide 250 μg/day, calcium citrate 2 g/day, etoricoxib 90 mg/day and assisted walking with walker at eight weeks with partial weight bearing.

Figure 1: Initial radiograph (left side), continuity solution at femoral diaphysis is observed with oblique tract, dislodged, without comminution, and cortical thickening. One day after (right side) closed reduction internal fixation with antegrade locked intramedullary nailing.
Two months later, she had a central densitometry, its reports: column L2-L4 BMD of 0.930 g/cm2 T-score -2.3, Z-score -0.7; in total BMD of 0.959, T-score -0.4, Z-score 0.8; X-ray examination of the contralateral femur show proximal lateral periosteal thickening (Figure 2).

Figure 2: Anteroposterior and lateral radiograph of the left femur, showing incomplete atypical fracture with proximal lateral cortical thickening.
On June 15, 2016 she was on full weight bearing without assistance, hip and knee with complete range of motion without instability.
On September 28, 2016, she had radiographic control of the right femur, with parcial bone healing (Figure 3), on the left femur presented with decreased lateral thickening (Figure 4), accordingly an atypical femoral fracture secondary to bisphosphonate intake was diagnosed.

Discussion
Bisphosphonates (BFs) are the initial therapy for osteoporosis, analogues of inorganic pyrophosphate, inhibits osteoclast activity and bone resorption.4 Two types of BFs: nitrogenated and non-nitrogenated. Non-nitrogenated: clodronate, etidronate and tiludronate. The nitrogenated: alendronate, ibandronate, risedronate, pamidronate and zoledronate.5
BFs have adverse bone effects: musculoskeletal pain, oversupression of bone remodeling, atypical fractures, maxillary osteonecrosis; and extra-osseous: gastroesophageal, ophthalmic, renal, hypocalcemia and atrial fibrillation.3
Atypical femoral fractures (AFFs): A stress fracture is due to an abnormal load in a normal bone, while one due to insufficiency is due to the normal load in an abnormal bone.2 The American Society of Bones and Minerals (ASBMR) concluded that AFFs are fractures of effort or insufficiency that progress over time.2 When a complete fracture occurs, the endochondral ossification is activated, the BFs interfere with the remodeling phase, delay the remodeling of callus from calcified cartilage to mature bone. With this suppression, intracortical repair of developing fatigue fractures decreases and microfractures can grow to a critical size.2
They are more common in the lower limbs because of the increased load and the geometry of the proximal femur, correlating with the deviation between the anatomical axis and the mechanical axis,2 producing a lateral transverse rupture, characteristic of a brittle material.6
The pathophysiology of AFFs is unknown, a series of mechanisms are suspected: microcracks accumulation, increase and reduction of bone mineralization heterogeneity, reduction of vascularity and antiangiogenic effects, accumulation of advanced glycation, reticular alteration, generating alterations in bone remodeling.7
The first report was given in 2005 with Odvina et al.8 In 2013 the ASBMR published the definition of AFFs, four major features are required, that may or may not be accompanied by minor features:9
Major features: Fracture associated with minimal trauma; transverse orientation, can become oblique; complete or incomplete fractures that only affect the lateral cortex; the fractures are minimally with or without comminution; In fracture site with periosteal or lateral endosteal thickening.
Minor features: Increased cortical thickness of the femoral shaft; pain in the groin or thigh; fractures of incomplete or complete femoral shaft; delayed healing; localization along the femoral shaft.
The overall incidence could be estimated at 7.8/100,000 person-years for patients over 60 years of age. A recent study has shown that this incidence increases with the time of exposure to the drug, from 2/100,000 cases/year for every two years of use of bisphosphonates to 78 per 100,000 cases/year for every eight years of use of these drugs.10
The usual treatment in these fractures was immediate suppression of the antiresorptive and a correct initial reduction of the fracture.10 In the case of incomplete atypical subtrochanteric or femoral diaphyseal fracture with thigh pain, prophylactic intramedullary nailing is recommended. A prior conservative treatment period may be chosen, keeping the patient under limited load with the aid of a walking stick. If clinical and radiological improvement is not achieved after two to three months with this treatment, prophylactic intramedullary nailing is recommended.10
The ASBMR suggests for those women who do not have a high risk of fractures after 3-5 years of treatment, to stop using BFs for a period of two to three years with periodic revaluation.11 Teriparatide (TPTD), a recombinant form of parathyroid hormone (PTH) and an anti-osteoporotic agent with potent bone formation effects, improves bone healing with a great positive effect in curing this type of fracture.12 In our clinical case, the association between the prolonged use of bisphosphonates and atypical fracture of the femur is demonstrated once again, as well as its adequate evolution with medical management, intramedullary nailing, and rehabilitation.

