











 nova página do texto(beta)
nova página do texto(beta) Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Craniosynostosis (CS) is a condition associated with increased intracranial pressure (ICP) due to the premature fusion of cranial sutures leading to restriction in the growth of the brain1. The prevalence of increased ICP in children with syndromic CS due to multiple suture fusion varies 4070%2. It can be due to hydrocephalus, airway obstruction, craniocerebral disproportion, or abnormalities in the venous drainage of the brain2. Depending on all these reasons, complications ranging from mild symptoms to death may occur due to increased ICP. In CS, cranial vault expansion surgery is performed to provide the most appropriate conditions to maximize the optimal condition of the brain or to prevent high ICP.
Increased intracranial pressure (ICP) can lead to permanent neurological sequelae. In patients with CS with high ICP, it is crusial to accelerate ICP-lowering measures and to maintain adequate cerebral perfusion3. In the literature, studies on the measurement of ONSD accompanied by USG, which is a noninvasive method in the detection of ICP increase, started in the early 90s. Especially in the last decade, it has been used frequently in adult and pediatric intensive care units as well as in the operating room during the intraoperative period.
Monitoring of ICP is widely used for the treatment and evaluation of patients with CS, who have elevated ICP4. Although invasive methods are the gold standard for monitoring ICP increase, serious complications such as infection and bleeding may occur in these procedures5,6. Although there are less invasive methods for ICP monitoring in pediatric and neonatal patients, because of their disadvantages, bedside optic nerve sheath diameter (ONSD) on ocular ultrasonography (USG) has begun to be increasingly used by pediatricians and intensive care specialists in recent years as it is a noninvasive method6.
Here, we presented the importance of ultrasound-guided ONSD measurements, a noninvasive method, in the diagnosis of ICP and ICP monitoring before and immediately after craniectomy in a child with CS.
Case Report
An eight-month-old male patient with a weight of 10 kg, who was diagnosed with CS, was decided to be operated by the neurosurgery department. In the preoperative evaluation of the patient, no additional problems were observed in his medical history, laboratory findings, and seizure history. Following a three-hour of fasting, the patient was transferred to the operating room and standard anesthesia monitoring (pulse oximetry, electrocardiography, non-invasive blood pressure, end-tidal carbon dioxide, temperature, and bispectral index) (Spacelabs Medical, USA) was performed. Then, oropharyngeal airways, laryngeal masks, and other essential equipment at varying sizes were prepared for the probability of difficult intubation. After achieving mask ventilation, anesthesia was induced with IV atropine (0.01 μg/kg-1), midazolam (0.5mg), fentanyl (1μg/kg-1), and propofol (3mg/kg-1). Endotracheal intubation was successfully performed using a 3.5-mm uncuffed endotracheal tube. Confirmation of endotracheal tube placement was performed with capnography and lung auscultation. Before and after the surgery, USG-guided ONSD measurement was performed to follow the changes in ICP. Volume-controlled ventilation was performed, with a tidal volume and respiratory frequency maintaining normocapnia (EtCO2 32-35 mmHg). No problem arose in the follow-up of hemodynamics and oxygenation. Furthermore, gas concentration of inhaled anesthetics was closely monitored throughout the surgery to monitor possible changes.
Following intubation, anesthesia was maintained with remifentanil and propofol administered in intermittent bolus injection of 50:50 oxygen/air mixture titrated to bispectral index (BIS) value 5060. No muscle relaxant was used throughout the surgical procedure. Fluid management was performed by the administration of balanced electrolyte solution based on the calculation of the perioperative fluid eficits and basal fluid requirement of the patient.
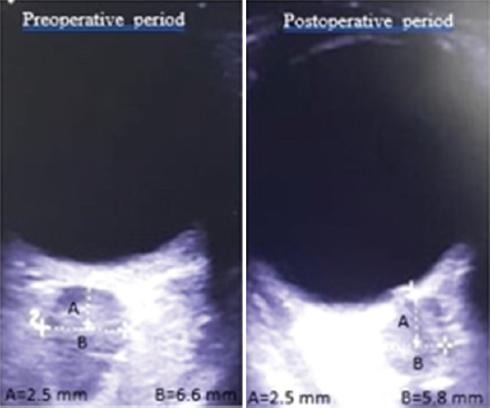
The ONSD value decreased from the preoperative value of 6.6 mm to the postoperative value of 5.8 mm (Fig. 1). During the surgical procedure, an appropriate surgical drape and skin sterilization were performed with the head flexed at 30 degrees while the patient was in the supine position and the skin was elevated in the form of a biparietal flap. Subgaleal dissection was performed without peeling the periosteum to keep the blood loss at the minimum level. The sagittal suture was removed by performing a 5-cm strip craniectomy. Barrel osteotomies were performed on the temporoparietal bones on both sides to expand the biparietal narrowing and suturectomy was performed on both coronal and lambdoid sutures. Then, frontal and occipital bones were reshaped by performing barrel osteotomies (Fig. 2). Surgical procedure lasted for 125 minutes and extubation was achieved uneventfully when the patient was full-awake. The patient was, then, transferred to the neonatal intensive care unit.

Discussion
Children with CS are at great risk for the development of increased ICP. The common clinical symptoms associated with increased ICP include headache, sleep disturbance, irritability, developmental delay, and decreased intellectual abilities7,8. Many underlying pathomechanisms have been reported related to the cause of increased ICP due to CS. Craniocerebral disproportion, hydrocephalus, abnormal venous drainage, and secondary extracranial factors are thought to affect ICP in these patients9,10.
Complications that may result in brain damage or even death as a result of cerebral ischemia and herniation due to uncontrolled ICP increase may occur. Monitoring of ICP is a clinically objective method that guides the physician in the evaluation and treatment of craniosynostosis. Furthermore, identifying patients with high ICP can help determine whether early intervention is required to prevent cognitive and neurological dysfunction.
In cases with CS, invasive ICP monitoring is widely used to confirm the suspicion of intracranial hypertension before performing corrective surgery3. Direct methods of ICP monitoring are the gold standard and are measured via epidural, subdural, and intraparenchymal intracranial catheter, as well as ventricular cannulation11. Conventional non-invasive methods used to determine ICP (e.g. Funduscopic examination, neuropsychiatric evaluation, bony changes on CT) often yield clear results12. In recent years, a new telemetric ICP monitoring system has been also used as a non-invasive and easy-to-apply method13. Although cranial magnetic resonance imaging or computed tomography is useful in the diagnosis of ICP in children, exposure to radiation for tomography imaging and the requirement for sedation in the pediatric age group are the disadvantages of these radiological examinations14. The fundoscopic examination is also very challenging for newborns since it requires pupil dilation and is impractical15,16.
Monitoring the changes is in ICP, which is one of the comorbidities that worsen the patient's condition before and after decompressive surgery, is of great importance. This will be guiding for the success of the surgery, as well as the patient's follow-up and treatment process. In monitoring these vital functions, there has been always a need for a minimally invasive and fast method of obtaining ICP measurements.
Bedside sonographic ophthalmic ultrasound measurement of ONSD is an easy, inexpensive, non-invasive, and reproducible technique that is commonly used in adults and children to detect ICP. One of the major advantages of this technique is that it does not expose the patient to any radiation7,17-19. The subarachnoid space is continuous with the optic nerve perineural space20. Changes in ONSD reflect the changes in ICP since there is a direct communication between the subarachnoid space and the optic nerve21. Increased ICP and increased CSF between the optic nerve and optic nerve sheath results in an enlarged ONSD since the cavity between the dura mater, optic nerve, and the optic nerve sheath is surrounded by the brain and cerebrospinal fluid22.
In the literature, there are many studies and meta-analyses investigating the normal value of ONSD in adult and pediatric age groups. Since the present case is included in the pediatric age group, the normal upper limit for ONSD has been reported to be 4.0 mm in children under one year of age and 4.5 mm in patients over one year of age23.
The present case report aimed to determine the level of preoperatively increased ICP in the early postoperative period and to reveal its clinical implications with serial ONSD measurements in an infant with CS undergoing craniectomy.
In the present case, measurements were performed preoperatively and postoperatively by placing a 7.5-MHz linear USG probe on the closed upper eyelid of the patient without excessive pressure after applying a thin layer of sterile gel at room temperature. Then, the ONSD was measured 2.5 mm behind the optic globe, from the transverse and sagittal planes. All measurements were performed twice, and the mean values were recorded.
Measurements showed that the postcraniectomy ONSD value was lower than the precraniectomy ONSD value (5.8 mm and 6.6 mm, respectively) (Fig. 1). This decrease in ONSD after craniectomy showed that ICP decreased and the surgery performed was effective.

