











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Connections between the esophagus and respiratory tract are uncommon entities; although very rare (3-11%), the esophageal pulmonary fistula (EPF) is a life-threatening condition.1-5 Other varieties of these connections are tracheal (52-57%) and bronchial (37-40%).1 Their origin may be congenital or acquired; and malignant (tracheal 15%, esophageal 5%, and lung 0.2%), or benign (infections, local trauma, Crohn’s disease, and chemo-or radiotherapy).1-5 The infections include tuberculosis, syphilis, histoplasmosis, actinomycosis and candidiasis.2 The commonest malignant causes are esophageal or bronchogenic cancers and lymphoma;2-4 and symptoms are coughing, dyspnea, recurrent infections, dysphagia and malnutrition.1,2,4,5 More effective local treatment is needed to reduce the mortality and get better quality of life.5 Surgical procedures, closure by clipping, and metallic or silicone stents are current options.2,5 As malignancies may evolve unsuspected or misinterpreted, diagnostic pitfalls often occur, in special because the clinical and routine radiological data can mimic pulmonary infections.1,3 The purpose of this report is to emphasize the role of autopsy in case of death of the patient.6
Case presentation
A 46-year-old female patient was admitted with loss of weight (10%), fever, cough and mucopurulent expectoration of two months of duration. She declared herself as a previously healthy and a never-smoker and denied the use of alcohol or illicit drugs, without exposure to biomass smoke or other main lung cancer risk factors. She had not chest surgery or radiotherapy, chemotherapy, airway invasion, or treatment of head and neck malignancy. On physical examination, pulmonary crackles were more clearly heard on the lower third of the right lung. Blood tests showed mild anemia, leukocytosis with neutrophilia and 12% of band forms. The other routine determinations were found within the respective normal parameters. Images of plain chest radiographs revealed parenchymal condensations with cavities (Figures 1A and 1B). Bronchoscopy showed edema and yellowish secretion in the bronchi of the right lower lobe and Klebsiella spp was identified in the aspirates, whereas malignant cells were not detected. The results of urine culture and repeated blood cultures were negative for microorganisms. She underwent general support measures and antibiotic therapy guided by sensitivity tests. Therefore, administered drugs of first option were amoxicillin associated with clavulanic acid; however, there was partial improvement of general clinical condition and the fever persisted. Furthermore, she presented repeated convulsive episodes associated with right hemiparesis, and her clinical status evolved to irreversible severe respiratory insufficiency, and expired. Necropsy study showed enlarged mediastinal lymph nodes and a cavitary mass in the lower lobe of the right lung with an esophageal-pulmonary fistula (Figure 2A). Histopathology study of tissue samples established the diagnosis of pulmonary carcinoma (Figure 2B) with infiltration of esophageal walls (Figure 2C), and metastasis to the cerebral cortex (Figure 2D).

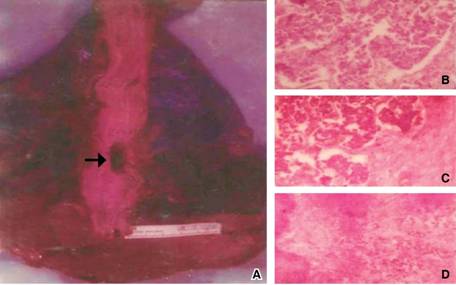
Figure 2: A: Gross view of the autopsy study revealing parenchymal changes in the right lung and the esophageal pulmonary fistula (arrow); and photomicrographs of main histopathologic findings: poorly differentiated lung carcinoma B esophageal wall infiltrated by malignant cells of lung cancer C and the evidence of metastasis in the central nervous system D.
Discussion
The never-smoker woman had an unsuspected primary lung cancer that evolved with invasion of the esophageal wall associated with a respiratory fistula; moreover, partial tumor necrosis with secondary infection mimicked a refractory excavated pneumonia by Klebsiella spp.1,3 Similarly to other descriptions, there was acute respiratory distress and multiorgan failure.2 On her admission, the major concern was about a possible pneumonia by bronchoaspiration. Clinical suspicion of esophageal fistula was impaired by the accentuated loss of appetite and almost exclusive ingestion of meals with liquid consistency during the most recent months. Actually, the very rapid and irreversible deterioration of the patient’s overall condition and her death prevented the accomplishment of complementary investigation by imaging exams.5 The scheduled evaluation, that might have given evidence of correct diagnoses included computed tomography of the chest, videofluoroscopy, and the upper digestive endoscopy.1,2,4 Worthy of note, the short survival time and lack of autopsy studies are often commented;1,2,4 however, the authorized postmortem evaluation enabled us to establish the correct diagnosis.
The complete autopsy allowed us to detect a metastatic lesion of lung cancer in the left brain hemisphere, which was related to the right hemiplegia presented few days before death. Neither cerebral bleeding nor remarkable signs of intracranial hypertension were observed, which can explain the lack of additional neurological changes except for convulsive episodes. There were also metastases in mediastinal and subcarinal lymph nodes, as well as in the liver. Immunohistochemistry studies showed negative stain for CK5/6, CK-10, CK-14, P63, TTF-1, and synaptophysin and positivity for CK-7 and CK-20; consistent with primary lung cancer.2,6 The negativity for P63 and CK5/6 in this scenery ruled out the squamous cells tumors, whereas the negativity for TTF-1 discarded the alternative hypothesis of an adenocarcinoma.2 The diagnosis was then a high-grade poorly differentiated carcinoma with large cell variant.6 Patients with highly aggressive undifferentiated type of this malignancy usually die in a short span of time after the onset of illness, and the diagnosis is often confirmed only at autopsy.6 Even without respiratory fistula, lung adenocarcinoma may also cause death in short periods.3 Differing from the findings disclosed in the present case study, primary esophageal cancer would have a profile with positivity for CK-10, CK-14, and negativity for CK-7 and CK-20.2
McCartney et al. reported a never-smoker 55-year-old man with delayed diagnosis of adenocarcinoma manifested as refractory pneumonia by Klebsiella, and progressing to death nine months after the initial presentation. Autopsy was not done, but the authors emphasized the advantages of targeted core pulmonary biopsies compared to the fine-needle aspirates. They also highlighted the frequent colonization of bronchial tree by Gram negative bacteria;3 phenomenon that may explain some diagnostic pitfalls involving pneumonia and lung cancer. The never-smoker status may have hindered the early diagnosis, as in the present case study. Duma et al. described an ever-smoker (20 pack-years) 61-year-old man with a bronchial-esophageal fistula due to a squamous cell carcinoma of the right lung diagnosed with base on bronchoscopic biopsy. Similar to the case herein described, there was acute respiratory distress and multiorgan failure; he died five days after admission, and autopsy was not done. The authors emphasized the rarity of this fistula as the initial presentation of lung carcinoma.2
Conclusion
Clinical and imaging data of the present case study were strongly indicative of a refractory community-acquired pneumonia with lung abscess caused by Klebsiella in a never-smoker. As a lung cancer associated with esophageal pulmonary fistula evolved unsuspected, the patient had a rapid downhill course during admission and died despite of clinical treatment. Case reports can confirm the main role of autopsy studies to put conundrums in evidence.

