










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkArchivos de cardiología de México
versión On-line ISSN 1665-1731versión impresa ISSN 1405-9940
Arch. Cardiol. Méx. vol.75 no.4 Ciudad de México oct./dic. 2005
Comunicaciones breves
Diverticulum of Kommerell
Divertículo de Kommerell
Juan Calderón–Colmenero,* Luis Muñoz,* José A García–Montes,* Samuel Ramírez, Emilia Patino,* Alfonso Buendía*
* Servicio de Cardiología Pediátrica.
Correspondence to:
Dr. Juan Calderón–Colmenero.
Instituto Nacional de Cardiología "Ignacio Chávez"
(INCICH Juan Badiano Núm. 1 Col. Sección XVI, Tlalpan,
14080 México, D.F.).
E–mail: juanecalderon@yahoo.com.mx
Recibido: 7 de julio de 2005
Aceptado: 12 de septiembre de 2005
Summary
A case of an 11–months–old girl with vomiting and laryngeal stridor is presented, and in whom a Kommerell diverticulum was demonstrated, which is a rare variant of the incomplete vascular ring. It is well known that the magnetic resonance is the best study to define this malformation. In this patient, it was the cardiac catheterization which allowed to define the structures that constituted the vascular ring. The patient was surgically treated in a successful way. The embryological knowledge of the transformations of the aortic arches offers great assistance in the understanding of all the types of vascular rings.
Key words: Kommerell's diverticulum. Vascular rings. Dysphagia.
Resumen
Se presenta el caso de lactante de 11 meses con historia de vómitos y estridor laríngeo secundaria a una rara variante de anillo vascular, divertículo de Kommerell. La resonancia magnética es considerada como el estudio ideal para definir la malformación, sin embargo, en este paciente, fue la angiografía la que permitió definir las estructuras del anillo vascular. El paciente fue tratado quirúrgicamente de manera exitosa. El conocimiento embriológico permite un adecuado entendimiento de los diferentes tipos de anillo vascular.
Palabras clave: Divertículo de Kommerell. Anillo vascular. Disfagia.
Introduction
The term vascular ring is referred to the alterations of the aortic arches in which the trachea and the esophagus are surrounded by these structures. They are divided in complete and partial; the former are the double aortic arch and the latter come from the aberrant origin of a subclavian artery, or arterial ligament or duct, counterside to the aortic arch. The symptoms and more characteristic signs are: persistent stridor and difficult feedings. The moment of the presentation is varied, but it normally occurs in the neonatal period.12 The purpose of this article is to present the case of a rare variant of the vascular ring with right aortic arch.
Presentation of the case
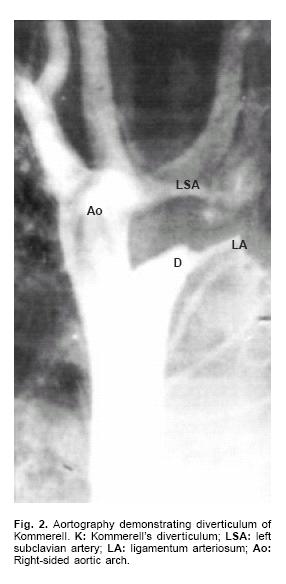
Female patient, 11 months old, referred to our Institute for vomits and laryngeal stridor occurring since the neonatal age. A barium esopha–gogram was carried out which showed right–sided indentation of the esophagus (Fig. 1). The echocardiogram did not find any intracardiac defect. The magnetic resonance did not defined accurately the structures which formed the vascular ring. The angiography showed right aortic arch from which the arteries emerged in this order: left brachycephalic arterial trunk situated on the left, right carotid artery and right subclavian artery. Left subclavian artery was pull by a ligament which began from a retroesophagic diverticulum from the descending aorta (Figs. 2–3). Surgical resection of the diverticulum, and section of the ligament was done so disappearing the digestive, and respiratory symptoms.


Discussion
The vascular rings represent less than 1% of all the cardiovascular malformations.1,2 This malformation is established for the persistence or the loss of specific segments from the rudimentary aortic arch. In the embryology of the aortic arch system, around the 36 to 38 days, six pairs of branchial arches originate six aortic arches with left–right symmetry, so constitute the primitive vascular back up of the brachycephalic structures.3,4
The embryonic aortic arches system are bilateral vessels which connect the ventral and dorsal aortas, this produces a bilateral vascular system that surrounds the fore gut intestine from which the trachea and the esophagus come from.
The distal parts of the first and second arches disappear close to the dorsal aorta, and the proximal areas of them close to the ventral aorta keep on as hyoid and maxillary arteries respectively, which are branches of the external carotid artery. The third aortic arches persist and form the proximal parts of the internal carotid arteries. On the other side the dorsal aorta between the third and fourth aortic arches known as carotid ducts, involute too. The fourth aortic arches persist encircling the anterior gut, this symmetry gives up an asymmetric pattern when one segment of the right dorsal aorta normally involutes between the seventh segmental artery and the place of union of both dorsal aortas which determines the formation of the aortic arch to the left. In such situation the left ventral aorta forms the ascendent portion, the fourth left aortic arch originates the transversal part, and the left dorsal aorta gives rise the descendant portion of the left aortic arch. The right ventral aorta give origin to the brachycephalic arterial trunk, from which the right common carotid artery and the right subclavian artery emerge, this last one has a tripartite origin, the proximal part derives from the right fourth aortic arch, the intermediate segment from the right dorsal aorta between this arch and the origin of the seventh segmentary artery, this last one constitutes the distal part.
The sixth aortic arches originate the proximal portions of the branches of the pulmonary artery and the right and left arterial ducts, the right one usually disappears and the left one keeps or remain patent during fetal life.
The Kommerell's diverticulum represents the persistency of the distal segment of double aortic arch, generally the left one which the proximal segment is atretic or disappears. Usually it is not associated with other congenital heart disease, some authors have reported the ventricular septal defect as the most frequent malformation, other series mention aortic coartation, tetralogy of Fallot and transposition of the great arteries.1–5,7
The clinical manifestations of the vascular ring and the seriousness will depend directly on the compression degree, in most of the patients the symptoms will appear before one month old, among the most known are the persistent stridor and feeding difficulty.2,6,7 The magnetic resonance is the best noninvasive techniques to demonstrate the anatomic features of vascular ring and thus to determine the optimal surgical approach. The cardiac catheterization is indicated when there is a confusion over the structures that form the vascular ring as it was in the case herewith. The surgical treatment is indicated in patients with symptoms of airway or esophageal compression. Cina reported a surgical mortality of 8.3% for elective treatment of Kommerell's aneurysm and Austin reported that 19% of affected patients presented with rupture, and all of them died.9–13
References
1. Van Son J, Julsrud P, Hagler D, Sim E: Surgical treatment of vascular rings: The Mayo Clinic experience. Mayo Clin Proc 1993; 68: 1056–1063. [ Links ]
2. Backer C, Ilbawi M, Idriss F: Vascular anomalies causing tracheoesophageal compression. Review of experience in children. J Thorac Cardiovasc Surg 1989; 97(5): 725–731. [ Links ]
3. Edwards J: Anomalies of derivatives of the aortic arch system. Mayo Clin North Am 1948; 32: 225–949. [ Links ]
4. Van Son J, Konstantinov I, Burckhard F: Kommerell and Kommerell's diverticulum. Texas Heart Inst J 2002; 29(2): 109–112. [ Links ]
5. Edwards J: Malformations of the aortic system manifested as vascular rings. Lav Invest 1953; 2: 56–75. [ Links ]
6. Rojas GE, Conejo ML, Cuenca PV, Maese HR, Sadeck A, Ferreiro M, et al: Dysphagia and stridor due to right aortic arch with Kommerell's diverticulum. AnnPediatr2004; 60(3): 288–289. [ Links ]
7. Buendía A, Calderón–Colmenero J, Patiño–Bahena E, Zabal C, Muñoz L, Attie F: Síndromes asociados a cardiopatías congénitas. PLAC Cardio 3. Intersistemas. México. 2002: 511–516. [ Links ]
8. McDougle L: Stridor in a 6 week old infant caused by right aortic arch with aberrant left subclavian artery. J Am Board Fam Pract 1999; 12(3): 219–224. [ Links ]
9. Morel V, Corbineau H, Lecoz A, Verhoye JP, Heautot JF, Basse R, et al: Two cases of "asthma" revealing a diverticulum of Kommerell. Respiration 2002; 69(5): 456–60. [ Links ]
10. Aoyagi S, Akashi H, Tayama K, Fujino T: Aneurysm of aberrant right subclavian (corrected) artery arising from diverticulum ofKommerell. Report of a case with tracheal compression. Eur J Cardiothorac Surg 1997; 12(1): 138–40. [ Links ]
11. Jung JY, Almond CH, Saab SB, Lababidi Z: Surgical repair of right aortic arch with aberrant left subclavian artery and left ligamentum arteriosum. J Thorac Cardiovasc Surg 1978; 75(2): 237–43. [ Links ]
12. Ciná CS, Althani H, Pasenau J, Abouzahy: Kommerell 's diverticulum and right–sided aortic arch: A cohort study and review of the literature. J Vase Surg 2004; 39: 131–9. [ Links ]
13. Austin EH, Wolfe GW: Aneurysm of aberrant subclavian artery with a review of the literature. J Vase Surg 1985; 2: 571–7. [ Links ]

