











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkA 74-year-old woman presented with weakness, dizziness, dyspnea, and chest pain. A 2nd degree atrioventricular block was found. Transvenous temporary pacemaker (TTP) was implanted. Post-TTP implantation electrocardiography (ECG) showed a paced rhythm with a right branch block (RBBB) morphology, inconsistent with the right ventricular stimulation as expected for this type of device. Chest X-ray showed the lead entering the right atrium through the superior vena cava, but the tip directed toward the left ventricular apex (Fig. 1). ECG pattern and location on chest X-ray suggested a left ventricle (LV) location of the electrode.
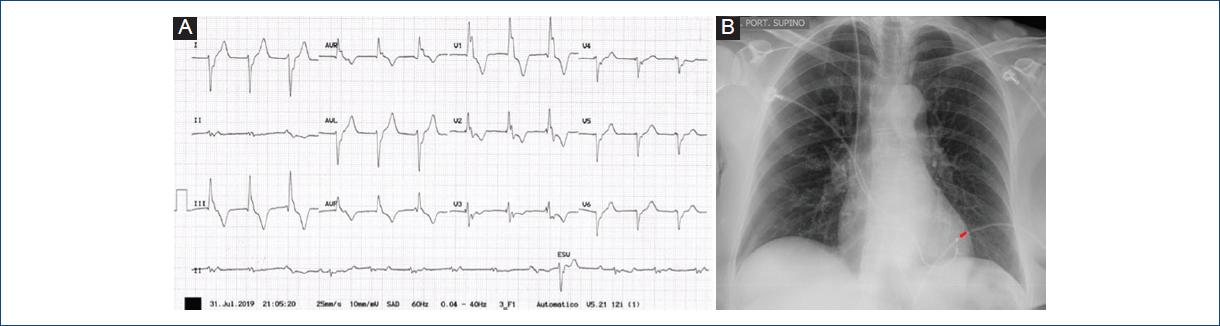
Figure 1 A: ECG: paced rhythm with a right branch block morphology. B: chest X-ray: lead in the right atrium with its tip directed toward the left ventricular apex (red arrow).
Transthoracic echocardiogram (TTE) documented a patent foramen ovale (PFO). The TTP lead crossed the PFO into the left atrium, and its distal segment formed a loop in the LV apex (Fig. 2).
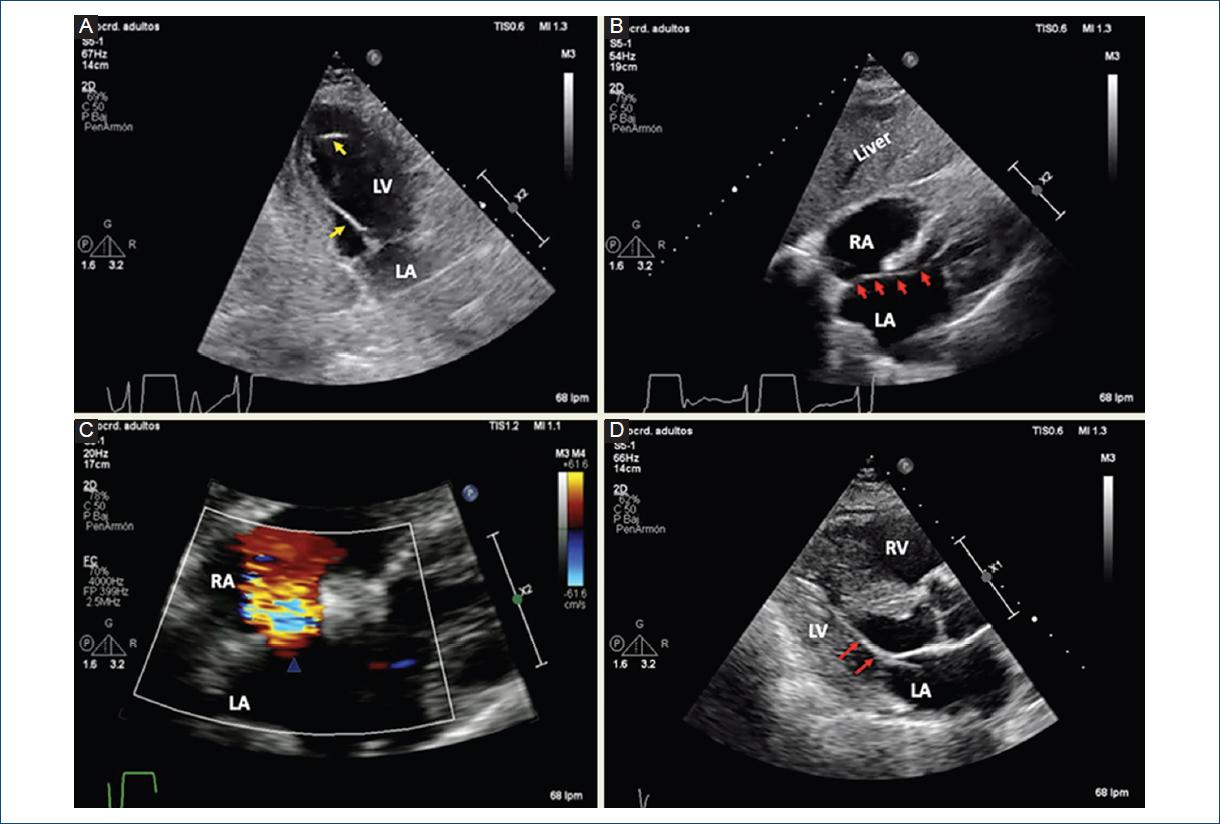
Figure 2 A: apical 2 chamber view: TTP lead forming a loop in the left ventricle apex (yellow arrow). B: subcostal 4 chamber view: TTP lead crossing through a PFO (red arrow). C: subcostal 4 chamber view: color Doppler at the interatrial septum (blue arrowhead). D: parasternal long-axis view: TTP lead in the left ventricle (red arrow). LA: left atria, LV: left ventricle, RA: right atria, RV: right ventricle.
TTP insertion is usually performed using ultrasound-guided venous punctures, but with blind electrode positioning. This procedure is considered safe and few complications are seen like as non-pericardial bleeding (2.4%), cardiac tamponade (0.6%), and iatrogenic pneumothorax (2.4%)1. Unnoticed stimulation of LV after a venous puncture is infrequent. The available data highlight the fortuitous passage of the lead through interatrial septum defects as a possible cause. Other possibilities include left ventricular location due to interventricular septum (IVS) perforation; RV apical location with depolarization vector going from left to right, in dilated cardiomyopathy, secondary to left displacement of the IVS and RV; and epicardial stimulation due to RV free wall perforation or by accessing LV coronary venous tributaries through the coronary sinus with presence of QS in D1 and aVL. The left location of these devices is a potential cause of embolism2.
A pacemaker stimulation with RBBB morphology after TTP insertion could help to predict the electrode location. Complementary studies such as chest X-ray, TTE, and fluoroscopy are useful to confirm the correct positioning of the electrode. The latter being less accessible to the patient’s bedside, but allowing the correct lead placement.

