











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Liver cancer is a public health problem in the world, since is the second leading cause of death and it is estimated that in 2012 produced 746,000 deaths (9.1% of all cancer deaths worldwide). In this same year, 782,000 new cases of LC in the world were estimated, affecting significantly less developed regions, where 83% of new cases of LC were observed, only in China 50% of cases were identified. LC is the fifth most common cause of cancer in men (554,000 cases, 7.5% of the total) and the ninth leading cause in women (228,000 cases, 3.4% of the total). The highest standardized incidence rates per 100,000 individuals in males were found in East and Southeast Asia (31.9 and 22.2, respectively). Intermediate incidence rates per 100,000 individuals were identified in southern Europe (9.5) and North America (9.3) and in the central and southern Asia region (3.7). The lowest LC incidence rates are in women. The highest rates in women are seen in eastern Asia and western Africa (10.2 and 8.1, respectively) and the lowest rates are found in northern Europe (1.9) and Micronesia (1.6)1.
In the world between 70 and 90% of primary liver cancers (PLC) correspond to hepatocellular carcinoma 2. Cholangiocarcinoma is the second most common of PLC, which accounts for up to 20% of PLC3. Cholangiocarcinomas mainly originate from the epithelial lining of the bile duct (intrahepatic and extrahepatic bile duct), but have high incidence rates in Thailand and some regions of Asia, due to the high prevalence in these regions of Fasciola hepatica infection. High rates of hepatocellular carcinoma in regions of Asia and sub-Saharan Africa, largely reflects the high prevalence of chronic infection with hepatitis B virus (HBV), with more than 5% of the population of these regions with chronic infection with HBV. In less developed countries the HBV and hepatitis C virus (HCV) are associated approximately with 32% of the cancers related to infections mostly liver cancer, and in the most developed countries are associated by 19%. Consumption of food contaminated with aflatoxin (a toxin produced by a fungus that infests grains, peanuts, soybeans and corn that have been stored in warm, moist conditions), is also a risk factor in less developed countries; however, the contribution of aflatoxin exposure to the burden of disease from LC in these countries is unknown. Other risk factors for hepatocellular carcinoma that are more common in Western countries include obesity, type 2 diabetes, cirrhosis related to heavy alcohol consumption, nonalcoholic fatty liver disease (associated with obesity), and smoking2.
Another very rare type of PLC is hepatoblastoma that have an annual incidence of 0.5-1.5 diagnoses per 1 million children age younger than 15 years in Western countries. After neuroblastoma and nephroblastoma, primary epithelial tumors of the liver are the third most common intraabdominal neoplasms in children. Hepatoblastoma is the most frequent liver tumor in Western countries. In Asia and Africa, hepatocellular carcinoma occurs more frequently than hepatoblastoma, probably as a consequence of the greater prevalence of hepatitis B infection on those continents4. Hepatoblastoma etiology is still unknown, most cases are sporadic whereas several genetic syndromes are associated with approximately 15% of cases and a close association with developmental syndromes such as the Beckwith-Wiedemann Syndrome and Familial Adenomatous Polyposis5.
In 2012 in Latin America, 63,160 cases of LC were reported, 40,288 men and 22,872 women (incidence rates: overall 5.3 per 100,000 population, men 7.4 and women 3.4) and that same year, 57,884 individuals died from this disease, 34,704 men and 23,180 women (mortality: overall 4.5 per 100,000 population, men 6.2 and women 3.3)6.
In Mexico the epidemiological information related to the LC is very scarce. In 2013 occurred 84,172 cancer deaths in Mexico, of these 6,594 (7.8%) were due to LC. In that year the LC ranked as the fourth leading cause of cancer death with a standardized mortality rate by age per 100,000 population of 7.8, after lung cancer (10.3), stomach (9.7) and prostate (8.3)7.
In Mexico there are no studies to investigate mortality trends from LC by state of residence and socioeconomic region and the risk of dying from LC according to the level of schooling and state of residence, so we consider carrying out this study could provide useful information.
The objective of this study was to determine mortality trends from LC by state and socioeconomic region and the risk of dying from LC according to the level of education and state of residence.
Materials and methods
An ecological study design was used. Mortality records associated to LC for 2000-2013 were obtained from the National Institute of Statistics and Geography8. This information is collected from death certificates issued nationwide. All individual records of mortality in which the basic cause of death was LC in the period of 2000 to 2013 were included in the study. The codes of the International Classification of Diseases, 10th revision were identified9. They corresponded to the basic cause of death from LC (C22.0-C22.9).
Raw and age-adjusted mortality rates nationwide per 100,000 inhabitants were obtained, taking the world population as the standard population10,11. Age-adjusted mortality rates per 100,000 inhabitants from each state and from each of the 7 socioeconomic regions (Table 1) established by the National Institute of Statistics and Geography were also obtained12. The national population, estimated by the National Population Council for 2000-201313, was used for the rate adjustment. The relative risk (RR) and 95% confidence interval (CI) were obtained by Poisson regression to determine the strength of association between educational attainment, and each one of the states of residence with the mortality from LC.
Table 1 Socioeconomic Regions of Mexico
| Socioeconomic Regions | States |
|---|---|
| 1 | Chiapas, Guerrero, Oaxaca |
| 2 | Campeche, Hidalgo, Puebla, San Luis Potosí, Tabasco, Veracruz |
| 3 | Durango, Guanajuato, Michoacan, Tlaxcala, Zacatecas |
| 4 | Colima, State of Mexico, Morelos, Nayarit, Querétaro, Quintana Roo, Sinaloa, Yucatan |
| 5 | Baja California, Baja California Sur, Chihuahua, Sonora, Tamaulipas |
| 6 | Aguascalientes, Coahuila, Jalisco, Nuevo Leon |
| 7 | Mexico City |
Source: National Institute of Statistics and Geography
The seven socioeconomic regional categories for Mexico have been defined by the National Institute of Statistics and Geography in which differences observed in the social and economic conditions of the population throughout México are presented according to the XII General Population and Housing Census. The seven socioeconomic regions comprise the 31 states and Mexico City according to indicators related to well-being such as education, occupation, health, housing and employment. States classified in the same region have similar characteristics on average; that is, they are homogenous, while the regions differ from one another. According to the indicators used, the socioeconomic conditions increase from Region 1, least favorable, to region 7 most favorable.
The methodology used to establish the regions had the objective of forming strata with minimal variance in an effort to group the elements more alike or closer to each other following a criterion of established similarity, which allows for differentiating one region from another. Among the techniques used are Mahalonobis distances and a combination of factorial analysis and the algorithm of the k-means12.
The Poisson regression model was chosen to determine the strength of association between state of residence, and educational level with mortality from liver cancer, because as a dependent variable, the number of deaths has a Poisson distribution that takes positive whole values. Poisson regression is equivalent to a logarithmic regression of mortality rates. The exponential coefficients allow for estimation of the RR of dying 14.
Registrations were handled by the Access 2013 program. The strength of association between educational level, and each state with mortality from LC were obtained by Poisson regression through the Number Cruncher Statistical System program 200115. The Epidat version 3.1 program was used to determine age-adjusted mortality rates by state, and socioeconomic region.
Results
In Mexico a total of 7,303,036 people died during the study period; of those deaths, 908,790 were due to a malignant neoplasms, 69,683 of which were LC. In the year 2000, there were 4,189 deaths from LC and in 2013, 5,755 individual died from this neoplasm. In the study period, the crude death rate per 100,000 people increased from 4.2 to 4.9 (percent change of 16.6%) (Fig. 1) and died for this cancer 32,745 men (47%) and 36,938 women (53%), with a male: female ratio of 0.88:1.0 (Table 2).

Figure 1 Mortality from liver cancer in Mexico. 2000-2013.Raw rate of mortality per 100,000 individualsAge-adjusted rate by the direct method, standardized with world population per 100,000 individuals.Source: Analysis by author from data taken from: the mortality database of the National Institute of Statistic and Geography and National Population Council: population estimates for the period 1990-2010 and population projections for the horizon 2010-2030.
Table 2 Deaths from liver cancer by site. México, 2000-2013
| ICD 10 code | Subset | Men Number (%) Deaths | Women Number (%) Deaths |
|---|---|---|---|
| C22.0 | Liver cell carcinoma | 9,334 (13.395) | 9, 104 (13.065) |
| C22.1 | Intrahepatic bile duct carcinoma | 2,354 (3.378) | 3,741 (5.369) |
| C22.2 | Hepatoblastoma | 237 (0.340) | 136 (0.195) |
| C22.3 | Angiosarcoma of liver | 20 (0.029) | 11 (0.016) |
| C22.4 | Other sarcomas of liver | 1 (0.001) | 6 (0.009) |
| C22.7 | Other specified carcinomas of liver | 238 (0.342) | 309 (0.443) |
| C22.9 | Malignant neoplasm of liver, not specified as primary or secondary | 20,550 (29.491) | 23,642 (33.928) |
| Total 32,734 (47) | Total 36,949 (53) |
In the study population, mortality from this disease increased with age. The highest mortality was identified in the group of 70-74 years old with 10,805 cases (15.5%) (Fig. 2). Trends in mortality rates in different age groups remained virtually unchanged, except for the age groups 51-60 years and 61-70 in which there was a decrease in mortality during the study period 2000-2013 (10.7-9.3 and 28.9-25.2, respectively); while individuals > 71 years, a slight increase in mortality from 61.9 to 62.1 was seen (Fig. 3).

Figure 2 Mortality from liver cancer by age. Mexico, 2000-2013.Source: Analysis by author from data taken from the mortality database of the National Institute of Statistic and Geography.
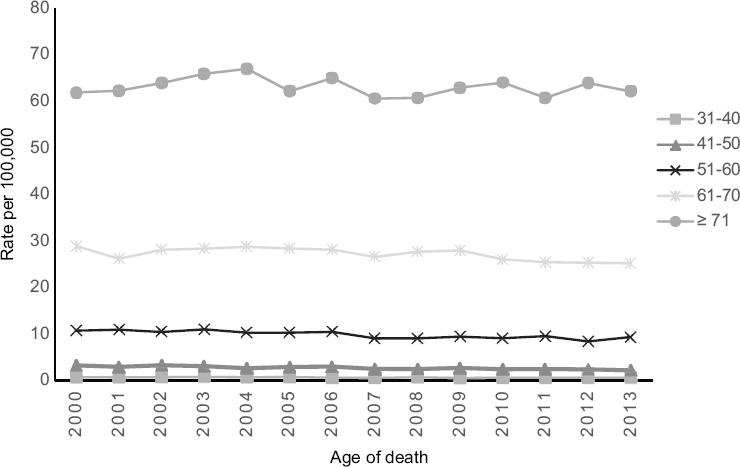
Figure 3 Mortality trends from liver cancer by age group. Mexico, 2000-2013.Mortality rate per 100,000 individuals.Source: Analysis by author from data taken from: the mortality database of the National Institute of Statistic and Geography and National Population Council: population estimates for the period 1990-2010 and population projections for the horizon 2010-2030.
The code C22.9 of ICD 10 (malignant neoplasm of liver, not specified as primary or secondary) was the most often recorded in patients with LC with 44,192 deaths and secondly, the code 22.0 (liver cell carcinoma) with 18,438 deaths. (Table 2).
In individuals with no schooling or with incomplete elementary school the relative risk (RR) of dying from LC was the highest (RR 8.61, 95% CI 8.35-8.89), while individuals with senior in high school or equivalent the RR decreased (RR 0.74, 95% CI 0.71 to 0.77) (Table 3).
Table 3 Relative risk (RR) of dying from liver cancer according to educational level, and 95% confidence interval (CI) according to Poisson regression. Mexico, 2000-2013
| Education | Relative Risk | 95% confidence Interval |
|---|---|---|
| No school or incomplete elementary school | 8.61 | 8.35-8.89 |
| Complete elementary school | 4.29 | 4.15-4.44 |
| High School or Equivalent | 0.90 | 0.86-0.94 |
| Senior in high school or equivalent | 0.74 | 0.71-0.77 |
| College | 1 | N.A |
Note: N/A: Not applicable.
In the study period, 22 states showed an increase in mortality, while 7 showed a decrease and there were no changes in 3 (considering the years 2000 and 2013) (Table 4). Chihuahua had the highest mortality rate, in 2000 the mortality rate in this state was 23, 95% CI 19.1-26.9 and in 2013, 19.1, 95% CI 15.8-22.3. The state had the lowest mortality rate was Colima, in 2000 and 2013 the rate was of 0.9 (Table 4).
Table 4 Age-adjusted mortality rate and 95% confidence interval by state of residence of individuals who died from liver cancer. México, 2000-2013
| States | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aguascalientes | 4.2 (2.9-5.6) | 3.6 (2.4-4.9) | 4.5 (3.1-5.9) | 3.1 (2-4.2) | 3.7 (2.4-4.9) | 3.1 (2-4.2) | 4.1 (2.8-5.4) | 4 (2.7-5.2) | 4.3 (3-5.6) | 3.2 (2.1-4.3) | 3.6 (2.4-4.7) | 3.6 (2.4-4.7) | 4.2 (2.9-5.4) | 3.5 (2.3-4.6) |
| Baja California | 3.4 (2.5-4.3) | 2.9 (2.2-3.7) | 3.9 (3-4.8) | 4.4 (3.5-5.3) | 3.9 (3.1-4.8) | 4.1 (3.2-4.9) | 4.3 (3.5-5.2) | 4.1 (3.2-4.9) | 3.1 (2.4-3.9) | 3.5 (2.8-4.2) | 3.9 (3.1-4.7) | 3.5 (2.8-4.2) | 4.2 (3.5-5) | 4.2 (3.5-5) |
| Baja California Sur | 2.4 (0.8-4) | 2.9 (1.2-4.6) | 5.1 (2.8-7.4) | 3.8 (1.9-5.7) | 5.4 (3.1-7.7) | 3.2 (1.5-4.8) | 5.6 (3.4-7.8) | 4.7 (2.7-6.8) | 2.9 (1.3-4.4) | 5.3 (3.2-7.3) | 2.5 (1.1-4) | 2.6 (1.2-4) | 3 (1.6-4.4) | 4.8 (2.9-6.7) |
| Campeche | 4.3 (2.7-5.9) | 4.8 (3.2-6.5) | 4.8 (3.1-6.4) | 3.9 (2.4-5.3) | 5.7 (3.9-7.4) | 4.9 (3.3-6.5) | 3.6 (2.2-4.9) | 5.3 (3.6-7) | 6 (4.2-7.7) | 4.6 (3.1-6.1) | 4.9 (3.3-6.4) | 4.6 (3.1-6.1) | 5.5 (3.9-7.2) | 6 (4.3-7.6) |
| Coahuila | 2.6 (2.1-3.2) | 2.9 (2.3-3.4) | 2.9 (2.4-3.5) | 2.9 (2.4-3.5) | 3 (2.4-3.5) | 2.9 (2.4-3.5) | 2.8 (2.2-3.3) | 3 (2.4-3.5) | 3 (2.4-3.5) | 3 (2.5-3.6) | 3.1 (2.5-3.7) | 2.6 (2.1-3.1) | 2.6 (2.1-3.1) | 2.6 (2.1-3.1) |
| Colima | 0.9 (0.6-1.3) | 0.6 (0.3-0.9) | 0.7 (0.4-1) | 0.9 (0.5-1.2) | 0.9 (0.6-1.3) | 0.6 (0.4-0.9) | 1.1 (0.7-1.4) | 0.6 (0.3-0.9) | 0.5 (0.3-0.8) | 0.8 (0.5-1.1) | 1.1 (0.7-1.5) | 0.8 (0.5-1.1) | 1 (0.6-1.3) | 0.9 (0.6-1.2) |
| Chiapas | 8.6 (7.3-9.8) | 9.1 (7.9-10.4) | 9.2 (8-10.5) | 9.6 (8.4-10.9) | 9.9 (8.7-11.2) | 9.3 (8.1-10.5) | 9.1 (7.9-10.3) | 9.7 (8.5-10.9) | 9.3 (8.1-10.5) | 11.2 (9.9-12.5) | 10.6 (9.4-11.9) | 11.8 (10.5-13.1) | 11.6 (10.3-12.9) | 12.9 (11.6-14.3) |
| Chihuahua | 23 (19.1-26.9) | 23.1 (19.2-27) | 21.8 (18.1-25.6) | 19.6 (16.1-23.1) | 19.7 (16.1-23.2) | 20.8 (17.2-24.4) | 21.8 (18.2-25.5) | 16.1 (13-19.2) | 18.1 (14.8-21.4) | 17.9 (14.7-21.2) | 14.9 (12-17.9) | 16.2 (13.2-19.3) | 18.3 (15.1-21.5) | 19.1 (15.8-22.3) |
| Mexico City | 4.4 (4-4.8) | 4.4 (4-4.8) | 4.4 (4-4.8) | 5 (4.6-5.4) | 4.7 (4.3-5.1) | 4.7 (4.3-5.1) | 4.7 (4.3-5.1) | 4.3 (3.9-4.7) | 4 (3.6-4.4) | 4.8 (4.4-5.2) | 4.7 (4.3-5.1) | 4.6 (4.2-5) | 4.6 (4.2-5) | 4 (3.6-4.3) |
| Durango | 4.3 (3.2-5.3) | 3.6 (2.6-4.6) | 3.6 (2.7-4.6) | 3.2 (2.3-4.1) | 4 (3-5) | 3.4 (2.5-4.3) | 3.4 (2.5-4.3) | 3.5 (2.6-4.5) | 3.8 (2.9-4.8) | 3.8 (2.9-4.8) | 2.9 (2.1-3.7) | 3.5 (2.6-4.4) | 3 (2.2-3.8) | 3.9 (3-4.8) |
| Guanajuato | 3.3 (2.7-3.8) | 3.1 (2.6-3.6) | 2.7 (2.3-3.2) | 3.6 (3-4.1) | 3.1 (2.6-3.6) | 2.8 (2.4-3.3) | 3.7 (3.2-4.2) | 2.9 (2.5-3.4) | 3.4 (2.9-3.9) | 3.1 (2.6-3.5) | 3.6 (3.1-4.1) | 3.6 (3.1-4.1) | 3.9 (3.4-4.4) | 3.7 (3.2-4.3) |
| Guerrero | 3 (2.4-3.6) | 2.4 (1.9-2.9) | 3.2 (2.6-3.8) | 3.5 (2.9-4.1) | 3.7 (3.1-4.4) | 3.2 (2.6-3.8) | 3.3 (2.7-3.9) | 3.4 (2.8-4) | 4.1 (3.4-4.8) | 4.7 (4-5.5) | 4.8 (4.1-5.6) | 3.4 (2.8-4) | 4 (3.3-4.7) | 3.5 (2.9-4.2) |
| Hidalgo | 2.9 (2.2-3.6) | 3.8 (3.1-4.6) | 4.4 (3.6-5.2) | 5.2 (4.3-6.1) | 4.1 (3.4-4.9) | 5.2 (4.3-6.1) | 4.7 >(3.9-5.6) | 4.8 (4-5.6) | 5 (4.2-5.9) | 5.7 (4.8-6.6) | 5.1 (4.2-5.9) | 4.4 (3.6-5.1) | 5.4 (4.5-6.2) | 5.9 (5-6.8) |
| Jalisco | 3.5 (3-3.9) | 3.5 (3.1-4) | 3.6 (3.1-4) | 3.7 (3.2-4.1) | 3.9 (3.4-4.3) | 3.5 (3.1-4) | 3.7 (3.3-4.2) | 3.6 (3.1-4) | 3.7 (3.3-4.1) | 3.4 (3-3.9) | 3.8 (3.3-4.2) | 3.6 (3.2-4) | 3.9 (3.4-4.3) | 3.1 (2.8-3.5) |
| State of Mexico | 4 (3.6-4.4) | 4 (3.6-4.3) | 3.9 (3.5-4.3) | 4.1 (3.7-4.5) | 3.9 (3.5-4.3) | 4.4 (4-4.7) | 4.4 (4-4.7) | 4.1 (3.8-4.5) | 4 (3.7-4.4) | 3.8 (3.5-4.2) | 4.1 (3.7-4.4) | 4.1 (3.7-4.4) | 4.1 (3.8-4.5) | 4.1 (3.8-4.4) |
| Michoacan | 3.5 (2.9-4) | 3.8 (3.3-4.4) | 3.8 (3.2-4.3) | 3.6 (3.1-4.2) | 4.1 (3.5-4.6) | 3.6 (3-4.1) | 3.9 (3.4-4.5) | 3.3 (2.8-3.9) | 3.5 (2.9-4) | 4.2 (3.6-4.8) | 4 (3.4-4.5) | 3.7 (3.2-4.3) | 3.7 (3.2-4.2) | 3.7 (3.2-4.3) |
| Morelos | 3.8 (2.9-4.7) | 3.6 (2.7-4.5) | 3.5 (2.6-4.4) | 3.9 (3-4.8) | 3.7 (2.9-4.6) | 3.6 (2.7-4.4) | 4 (3.1-4.8) | 4.4 (3.5-5.4) | 3.9 (3-4.8) | 5.7 (4.7-6.8) | 4.2 (3.3-5.1) | 4.2 (3.3-5.1) | 4.3 (3.4-5.2) | 4.6 (3.7-5.5) |
| Nayarit | 6.1 (4.6-7.5) | 4.1 (2.9-5.3) | 4.6 (3.3-5.8) | 4.7 (3.5-6) | 6 (4.6-7.5) | 5.8 (4.4-7.2) | 5.6 (4.2-6.9) | 4.1 (2.9-5.2) | 5.2 (3.9-6.5) | 5.2 (3.9-6.5) | 4.8 (3.6-6) | 4.3 (3.1-5.4) | 5.9 (4.6-7.3) | 4.6 (3.4-5.8) |
| Nuevo Leon | 4.3 (3.7-5) | 4.1 (3.4-4.8) | 4.1 (3.4-4.7) | 3.7 (3.1-4.3) | 3.3 (2.8-3.9) | 4.5 (3.9-5.2) | 4.7 (4-5.4) | 4 (3.4-4.6) | 3.8 (3.3-4.4) | 4.3 (3.7-4.9) | 4.5 (3.9-5.1) | 4.4 (3.8-5) | 4.4 (3.8-5) | 4.3 (3.7-4.9) |
| Oaxaca | 3.6 (3.1-4.2) | 3.5 (3-4.1) | 4.2 (3.6-4.8) | 4.4 (3.7-5) | 4.4 (3.8-5) | 4.1 (3.5-4.7) | 4.6 (3.9-5.2) | 5.1 (4.4-5.8) | 5.4 (4.7-6.1) | 5.3 (4.6-6) | 5 (4.4-5.7) | 5.8 (5.1-6.5) | 6.1 (5.3-6.8) | 5.3 (4.6-6) |
| Puebla | 3.5 (3-4) | 3.4 (2.9-3.9) | 3.8 (3.2-4.3) | 4.5 (3.9-5) | 4 (3.5-4.5) | 4.8 (4.2-5.3) | 4.8 (4.2-5.4) | 4 (3.5-4.5) | 4.7 (4.1-5.2) | 4.5 (4-5.1) | 4.7 (4.1-5.2) | 5.2 (4.6-5.8) | 4.8 (4.2-5.3) | 5.6 (5-6.2) |
| Queretaro | 3.1 (2.2-4.1) | 2.6 (1.8-3.5) | 2.8 (1.9-3.7) | 2.8 (1.9-3.7) | 2.6 (1.7-3.4) | 4.3 (3.2-5.3) | 4.5 (3.4-5.5) | 3.5 (2.6-4.5) | 4.9 (3.7-6) | 3.6 (2.7-4.6) | 3.6 (2.6-4.5) | 3.4 (2.5-4.3) | 3.8 (2.9-4.8) | 3.5 (2.6-4.4) |
| Quintana Roo | 3.9 (2.1-5.6) | 4 (2.3-5.7) | 5.3 (3.3-7.4) | 4.1 (2.4-5.8) | 4 (2.3-5.7) | 5 (3.2-6.8) | 4 (2.3-5.6) | 3.8 (2.3-5.4) | 4 (2.5-5.5) | 3.9 (2.4-5.4) | 4.2 (2.7-5.7) | 4.9 (3.2-6.5) | 5.6 (3.9-7.3) | 5.2 (3.6-6.8) |
| San Luis Potosi | 4.2 (3.5-5) | 3.9 (3.2-4.7) | 3.8 (3.1-4.6) | 4.8 (4-5.7) | 5.8 (4.9-6.7) | 4.8 (4-5.7) | 4.9 (4.1-5.7) | 6 (5.1-6.9) | 5 (4.2-5.8) | 5.2 (4.4-6.1) | 5.4 (4.6-6.3) | 6.1 (5.2-7) | 5.4 (4.5-6.2) | 6.3 (5.4-7.2) |
| Sinaloa | 5.1 (4.2-5.9) | 3.5 (2.8-4.3) | 4.2 (3.4-5) | 4.1 (3.3-4.8) | 5.1 (4.2-5.9) | 4.7 (3.9-5.5) | 4.4 (3.6-5.1) | 3.5 (2.8-4.2) | 4.6 (3.8-5.4) | 4 (3.3-4.7) | 3.8 (3.1-4.5) | 3.8 (3.1-4.5) | 4.2 (3.5-5) | 3.2 (2.6-3.9) |
| Sonora | 3.6 (2.8-4.4) | 4.5 (3.6-5.5) | 3.9 (3.1-4.7) | 4.9 (4-5.8) | 3.8 (3-4.6) | 4 (3.2-4.9) | 3.7 (3-4.5) | 2.9 (2.2-3.6) | 3.4 (2.7-4.2) | 4.2 (3.4-4.9) | 4.2 (3.4-5) | 3.8 (3.1-4.6) | 4 (3.3-4.8) | 4.7 (3.9-5.5) |
| Tabasco | 4.8 (3.8-5.9) | 5.5 (4.4-6.7) | 6.1 (4.9-7.3) | 5.4 (4.3-6.5) | 5.6 (4.5-6.7) | 5.3 (4.3-6.4) | 6.3 (5.1-7.4) | 5.7 (4.6-6.8) | 6.6 (5.4-7.8) | 6.2 (5.1-7.4) | 6 (4.9-7.1) | 6.2 (5.1-7.4) | 6.6 (5.4-7.7) | 7.6 (6.4-8.8) |
| Tamaulipas | 5.6 (4.7-6.5) | 6.2 (5.3-7.1) | 6.6 (5.7-7.6) | 5.9 (5-6.8) | 5.7 (4.8-6.6) | 5.4 (4.6-6.2) | 6.6 (5.7-7.5) | 5.4 (4.6-6.2) | 6.3 (5.4-7.1) | 6 (5.2-6.9) | 7.4 (6.5-8.4) | 6.4 (5.5-7.2) | 6.1 (5.3-7) | 5.8 (5-6.6) |
| Tlaxcala | 2.7 (1.7-3.7) | 2.3 (1.3-3.2) | 3.6 (2.4-4.7) | 4 (2.8-5.2) | 2.9 (1.9-3.9) | 2.1 (1.2-2.9) | 4.6 (3.3-5.9) | 3.6 (2.5-4.7) | 3.1 (2.1-4.1) | 4 (2.8-5.2) | 3.8 (2.6-4.9) | 2.8 (1.8-3.8) | 3.5 (2.4-4.6) | 4.6 (3.3-5.8) |
| Veracruz | 5.9 (5.4-6.5) | 6.1 (5.6-6.7) | 6.8 (6.2-7.3) | 6.7 (6.2-7.3) | 7.5 (6.9-8) | 7.2 (6.6-7.8) | 7.2 (6.6-7.7) | 6.7 (6.1-7.2) | 7 (6.5-7.6) | 7.5 (7-8.1) | 7.4 (6.8-8) | 7.6 (7-8.1) | 7.4 (6.9-8) | 8 (7.4-8.6) |
| Yucatan | 6.4 (5.3-7.5) | 5.8 (4.7-6.8) | 5.8 (4.7-6.9) | 6.6 (5.5-7.8) | 6.4 (5.3-7.5) | 5.8 (4.7-6.8) | 5.6 (4.5-6.6) | 6.5 (5.4-7.6) | 5.9 (4.9-6.9) | 6.1 (5.1-7.2) | 5.8 (4.7-6.8) | 7.4 (6.3-8.6) | 7 (5.9-8.1) | 8.2 (7.1-9.4) |
| Zacatecas | 3.1 (2.3-4) | 3.9 (3-4.9) | 4.1 (3.1-5.1) | 3.8 (2.9-4.8) | 4.3 (3.3-5.3) | 3.5 (2.6-4.4) | 3.6 (2.7-4.5) | 2.9 (2.1-3.8) | 3.5 (2.6-4.4) | 3.3 (2.4-4.2) | 3.8 (2.9-4.7) | 3.3 (2.4-4.1) | 3.2 (2.3-4.1) | 4.8 (3.8-5.9) |
Rate per 100,000 inhabitants adjusted by direct method using national population as standard population. Source: Analysis by author from data taken from: the mortality database of the National Institute of Statistic and Geography and National Population Council: population estimates for the period 1990-2010 and population projections for the horizon 2010-2030.
The socioeconomic region 2 had the highest mortality rate from LC. In 2000 the mortality rate for this region was 5.2, 95% CI 4.9-5.5 and in 2013 was 7.8, 95% CI 7.4-8.1. There were no region with the lowest mortality for several years in the period 2000-2013 (Table 5). The regions with the lowest mortality in the study period were region 1 (2000, 2001), region 3 (2002-2005, 2007-2012), region 6 (2013) and the region 1 and 3 (2006). The mortality rate from LC for region 1 in 2000 and 2001 was 3.3, 95% CI 3-3.6 and 3.2, 95% CI 2.9-3.5, respectively; for region 3 in 2002 and 2012 was 3.4, 95% CI 3.1-3.7 and 3.6, 95% CI 3.3-3.9, respectively; for region 6 in 2013 was 3.6, 95% CI 3.3-3.9; for region 1 and 3 in 2006 the mortality rate was 3.8, CI95 3.5-4.1 (Table 5).
Table 5 Age-adjusted mortality rate and 95% confidence intervals (CI) by socioeconomic region of individuals who died from liver cancer. México, 2000-2013
| Region | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 3.3 (3-3.6) | 3.2 (2.9-3.5) | 3.6 (3.3-3.9) | 3.9 (3.5-4.2) | 4 (3.6-4.3) | 3.7 (3.4-4) | 3.8 (3.5-4.1) | 4.1 (3.8-4.4) | 4.3 (4-4.7) | 4.8 (4.4-5.1) | 4.6 (4.2-4.9) | 4.7 (4.4-5.1) | 4.9 (4.5-5.2) | 4.9 (4.5-5.2) |
| 2 | 5.2 (4.9-5.5) | 5.4 (5.1-5.8) | 5.9 (5.6-6.3) | 6.3 (5.9-6.6) | 6.5 (6.2-6.9) | 6.6 (6.2-7) | 6.6 (6.2-7) | 6.3 (6-6.7) | 6.7 (6.3-7) | 6.9 (6.5-7.3) | 6.8 (6.4-7.2) | 7 (6.7-7.4) | 7 (6.6-7.3) | 7.8 (7.4-8.1) |
| 3 | 3.4 (3.1-3.7) | 3.4 (3.1-3.7) | 3.4 (3.1-3.7) | 3.6 (3.3-3.9) | 3.6 (3.3-4) | 3.2 (2.9-3.5) | 3.8 (3.5-4.1) | 3.2 (2.9-3.5) | 3.4 (3.1-3.8) | 3.6 (3.3-4) | 3.7 (3.4-4) | 3.5 (3.2-3.8) | 3.6 (3.3-3.9) | 3.9 (3.6-4.3) |
| 4 | 4.4 (4.1-4.7) | 3.9 (3.7-4.2) | 4 (3.8-4.3) | 4.3 (4-4.5) | 4.3 (4-4.6) | 4.5 (4.3-4.8) | 4.5 (4.2-4.8) | 4.2 (4-4.5) | 4.3 (4.1-4.6) | 4.3 (4-4.5) | 4.2 (4-4.5) | 4.3 (4-4.6) | 4.5 (4.3-4.8) | 4.4 (4.2-4.7) |
| 5 | 4.5 (4-4.9) | 4.7 (4.3-5.1) | 4.9 (4.5-5.3) | 4.8 (4.4-5.3) | 4.5 (4.1-4.9) | 4.5 (4.1-4.8) | 4.9 (4.5-5.3) | 4 (3.6-4.4) | 4.2 (3.8-4.6) | 4.4 (4-4.8) | 4.6 (4.2-5) | 4.2 (3.9-4.6) | 4.5 (4.1-4.9) | 4.6 (4.3-5) |
| 6 | 3.9 (3.5-4.2) | 3.8 (3.5-4.1) | 3.9 (3.6-4.3) | 3.7 (3.4-4) | 3.8 (3.5-4.1) | 3.9 (3.6-4.2) | 4.1 (3.8-4.4) | 3.8 (3.5-4.1) | 3.9 (3.6-4.2) | 3.8 (3.5-4.1) | 4.1 (3.8-4.4) | 3.9 (3.6-4.2) | 4 (3.7-4.3) | 3.6 (3.3-3.9) |
| 7 | 4.4 (4-4.8) | 4.4 (4-4.8) | 4.4 (4-4.8) | 5 (4.6-5.4) | 4.7 (4.3-5.1) | 4.7 (4.3-5.1) | 4.7 (4.3-5.1) | 4.3 (3.9-4.7) | 4 (3.6-4.4) | 4.8 (4.4-5.2) | 4.7 (4.3-5.1) | 4.6 (4.2-5) | 4.6 (4.2-5) | 4 (3.6-4.3) |
Rate per 100,000 inhabitants adjusted by direct method using national population as standard population.
Source: Analysis by author from data taken from: the mortality database of the National Institute of Statistic and Geography and National Population Council: population estimates for the period 1990-2010 and population projections for the horizon 2010-2030.
Chihuahua had the highest RR of dying from LC, in 2000 the RR was 30.3, 95% CI 19.6-46.8 and in 2013 the RR was 22.3, 95% CI 15.1-33 (Table 6). There was no state with the lowest relative risk of dying for several years during the study period, the states with the lowest RR of dying from LC were Baja California Sur (2000, 2010, 2011), Baja California (2001), Coahuila (2002, 2008, 2012, 2013), Quintana Roo (2003, 2004, 2006, 2007, 2009) and Tlaxcala (2005). Baja California Sur had a RR in 2000 and 2011 of 2.4, 95% CI 1.1-5.2 and RR 2.7, 95% CI 1.4-5.2, respectively; Baja California in 2001 had a RR 4.2, 95% CI 2.4-7.3; Coahuila in 2002 and 2013 had a RR of 3.9, 95% CI 2.4-6.4 and RR 2.4, 95% CI 1.6-3.6, respectively; Quintana Roo in 2003 and 2009 had a RR of 2.8, 95% CI 1.6-4.9 and RR 3, 95% CI 1.7-5.1, respectively; Tlaxcala in 2005 had a RR of 3.3, 95% CI 1.8-6 (Table 6).
Table 6 Relative risk (RR) of dying from liver cancer by state and 95% confidence interval (CI), according to Poisson Regression, Mexico, 2000-2013
| ENTIDAD | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aguascalientes | 4.6 (2.7-7.6) | 5.9 (3.3-10.8) | 6.4 (3.7-11.1) | 3.5 (2-5.9) | 3.8 (2.3-6.2) | 4.3 (2.4-7.6) | 3.5 (2.2-5.6) | 6 (3.4-10.3) | 7.5 (4.3-13.2) | 3.8 (2.2-6.4) | 2.9 (1.9-4.7) | 4 (2.4-6.6) | 3.9 (2.5-6.1) | 3.5 (2.2-5.6) |
| Baja California | 3.2 (2-5.1) | 4.2 (2.4-7.3) | 4.8 (2.9-7.9) | 4.2 (2.7-6.6) | 3.6 (2.3-5.6) | 5.2 (3.2-8.4) | 3.4 (2.3-5) | 5.4 (3.3-8.9) | 4.9 (2.9-8.3) | 4 (2.5-6.2) | 3 (2.1-4.4) | 3.6 (2.3-5.5) | 3.7 (2.5-5.4) | 4 (2.7-5.9) |
| Baja California Sur | 2.4 (1.1-5.2) | 4.4 (2-9.4) | 6.3 (3.3-11.8) | 3.7 (2-7) | 4.7 (2.7-8.4) | 4.2 (2.1-8.3) | 4.5 (2.6-7.5) | 6.4 (3.4-11.9) | 4.7 (2.3-9.5) | 5.6 (3.2-9.7) | 1.8 (0.9-3.5) | 2.7 (1.4-5.2) | 2.7 (1.5-4.8) | 4.2 (2.5-7.2) |
| Campeche | 5.2 (3-8.8) | 8.8 (4.8-16) | 7.4 (4.2-13) | 4.6 (2.7-7.9) | 6.3 (3.9-10.3) | 7.5 (4.3-12.9) | 3.3 (2-5.6) | 8.7 (5-15.1) | 11.2 (6.4-19.6) | 5.9 (3.5-9.9) | 4.4 (2.8-7) | 5.6 (3.4-9.2) | 5.5 (3.5-8.7) | 6.4 (4.1-10) |
| Chiapas | 9.9 (6.5-15.1) | 16 (9.6-26.6) | 14 (8.7-22.3) | 11.4 (7.6-17.3) | 11.1 (7.5-16.6) | 14.3 (9.1-22.7) | 8.7 (6-12.5) | 16.2 (10.2-25.9) | 18 (11-29.4) | 14.9 (9.9-22.5) | 9.9 (7-14) | 15 (10.1-22.2) | 12.1 (8.5-17.4) | 14.7 (10.2-21.3) |
| Chihuahua | 30.3 (19.6-46.8) | 45.8 (27.2-76.8) | 37.3 (23-60.3) | 26.4 (17.2-40.6) | 24.7 (16.3-37.5) | 35.2 (22-56.5) | 22.6 (15.5-33.1) | 29.4 (18-47.9) | 37.1 (22.3-61.8) | 25.3 (16.4-38.9) | 14.7 (10-21.5) | 21.6 (14.2-32.9) | 19.9 (13.6-29.2) | 22.3 (15.1-33) |
| Coahuila | 2.7 (1.7-4.2) | 4.4 (2.6-7.5) | 3.9 (2.4-6.4) | 2.9 (1.9-4.5) | 2.8 (1.8-4.2) | 3.9 (2.4-6.3) | 2.2 (1.5-3.3) | 4.1 (2.5-6.7) | 4.7 (2.8-7.8) | 3.3 (2.1-5.1) | 2.4 (1.6-3.4) | 2.7 (1.8-4.2) | 2.2 (1.5-3.2) | 2.4 (1.6-3.6) |
| Mexico City | 6.2 (4.1-9.4) | 9.7 (5.9-15.9) | 8.4 (5.3-13.3) | 7.6 (5.1-11.3) | 6.7 (4.6-9.9) | 9.4 (6-14.6) | 5.8 (4.1-8.3) | 9.4 (6-14.9) | 10.1 (6.2-16.4) | 8.5 (5.7-12.6) | 5.8 (4.1-8.1) | 7.8 (5.3-11.5) | 6.4 (4.5-9.2) | 6 (4.2-8.7) |
| Durango | 5.2 (3.3-8.4) | 6.7 (3.8-11.7) | 5.8 (3.4-9.8) | 4 (2.5-6.5) | 4.8 (3-7.5) | 5.6 (3.4-9.4) | 3.5 (2.3-5.4) | 6.3 (3.8-10.6) | 7.8 (4.6-13.3) | 5.4 (3.4-8.6) | 2.9 (1.9-4.4) | 4.7 (3-7.4) | 3.4 (2.2-5.2) | 4.6 (3-7.1) |
| Guanajuato | 3.9 (2.5-6) | 5.8 (3.5-9.7) | 4.4 (2.7-7.1) | 4.4 (2.9-6.6) | 3.6 (2.4-5.4) | 4.5 (2.8-7.2) | 3.6 (2.5-5.3) | 5.1 (3.2-8.2) | 6.6 (4-10.9) | 4.1 (2.7-6.3) | 3.4 (2.4-4.8) | 4.6 (3-6.8) | 4.1 (2.8-5.9) | 4.2 (2.9-6.1) |
| Guerrero | 4 (2.6-6.3) | 4.8 (2.8-8.2) | 5.5 (3.4-8.9) | 4.6 (3-7.1) | 4.7 (3.1-7.1) | 5.5 (3.4-8.9) | 3.5 (2.3-5.1) | 6.4 (3.9-10.3) | 8.7 (5.3-14.4) | 6.9 (4.5-10.5) | 4.8 (3.4-6.9) | 4.6 (3-7) | 4.5 (3.1-6.6) | 4.3 (2.9-6.3) |
| Hidalgo | 3.9 (2.4-6.1) | 7.9 (4.7-13.4) | 7.7 (4.8-12.6) | 7 (4.6-10.7) | 5.2 (3.4-8) | 9 (5.6-14.4) | 5.1 (3.4-7.4) | 9.1 (5.6-14.7) | 10.7 (6.5-17.7) | 8.3 (5.5-12.7) | 5.2 (3.6-7.6) | 6 (3.9-9.1) | 6.1 (4.2-8.8) | 7.2 (4.9-10.5) |
| Jalisco | 4.6 (3-7) | 7.1 (4.3-11.7) | 6.1 (3.8-9.8) | 4.9 (3.2-7.3) | 4.8 (3.2-7.1) | 5.9 (3.8-9.4) | 3.9 (2.7-5.6) | 6.5 (4.1-10.4) | 7.6 (4.7-12.4) | 4.9 (3.2-7.4) | 3.7 (2.6-5.3) | 4.8 (3.2-7.1) | 4.2 (2.9-6.1) | 3.7 (2.5-5.4) |
| State of Mexico | 3.9 (2.6-5.9) | 6.1 (3.7-10) | 5.1 (3.2-8.1) | 4.2 (2.8-6.3) | 3.8 (2.6-5.6) | 5.9 (3.8-9.2) | 3.6 (2.6-5.2) | 6.1 (3.9-9.6) | 6.8 (4.2-11) | 4.5 (3-6.8) | 3.4 (2.4-4.8) | 4.6 (3.1-6.7) | 3.9 (2.8-5.5) | 4.2 (2.9-6) |
| Michoacan | 5 (3.2-7.6) | 8.4 (5-14) | 7.1 (4.4-11.3) | 5.2 (3.4-7.9) | 5.6 (3.7-8.3) | 6.7 (4.2-10.7) | 4.5 (3.1-6.5) | 6.8 (4.2-10.9) | 7.8 (4.7-12.8) | 6.6 (4.3-9.9) | 4.4 (3.1-6.2) | 5.5 (3.7-8.2) | 4.4 (3-6.4) | 4.8 (3.3-7) |
| Morelos | 5.2 (3.3-8.4) | 7.7 (4.4-13.3) | 6.3 (3.8-10.6) | 5.5 (3.5-8.6) | 5 (3.2-7.8) | 6.6 (4-10.9) | 4.5 (3-6.8) | 8.8 (5.4-14.5) | 8.9 (5.2-15) | 8.9 (5.8-13.8) | 4.6 (3.1-6.7) | 6.1 (4-9.5) | 5.2 (3.5-7.8) | 6 (4-9) |
| Nayarit | 8.9 (5.6-14.2) | 9.3 (5.2-16.3) | 8.9 (5.2-15) | 7 (4.4-11.3) | 8.2 (5.3-12.9) | 10.8 (6.6-17.8) | 6.3 (4.2-9.7) | 8.2 (4.8-14) | 11.6 (6.8-19.9) | 8.1 (5.1-12.9) | 5.1 (3.4-7.8) | 6.1 (3.8-9.6) | 7 (4.6-10.5) | 5.8 (3.7-8.9) |
| Nuevo Leon | 4.9 (3.2-7.6) | 7.2 (4.3-12) | 6.1 (3.8-9.9) | 4.3 (2.8-6.5) | 3.7 (2.4-5.6) | 7 (4.4-11.1) | 4.4 (3.1-6.4) | 6.7 (4.2-10.8) | 7.4 (4.5-12.2) | 5.8 (3.8-8.7) | 4.2 (3-6) | 5.6 (3.8-8.4) | 4.7 (3.2-6.7) | 4.9 (3.4-7.2) |
| Oaxaca | 5.4 (3.5-8.3) | 8.1 (4.9-13.6) | 8.4 (5.2-13.4) | 6.5 (4.3-9.9) | 6.2 (4.2-9.3) | 7.9 (5-12.6) | 5.4 (3.8-7.9) | 10.6 (6.7-17) | 12.8 (7.8-20.9) | 8.5 (5.7-12.9) | 5.7 (4-8.1) | 8.6 (5.8-12.8) | 7.4 (5.2-10.7) | 7.1 (4.8-10.3) |
| Puebla | 4.4 (2.9-6.8) | 6.6 (4-11.1) | 6.3 (3.9-10) | 5.8 (3.8-8.7) | 4.8 (3.2-7.2) | 7.8 (5-12.4) | 4.9 (3.4-7) | 7.1 (4.5-11.4) | 9.5 (5.8-15.4) | 6.3 (4.2-9.5) | 4.5 (3.2-6.4) | 6.8 (4.6-10) | 5.1 (3.6-7.4) | 6.4 (4.4-9.2) |
| Queretaro | 3.4 (2-5.6) | 4.3 (2.4-7.8) | 4 (2.3-6.9) | 3 (1.8-5) | 2.6 (1.6-4.3) | 6 (3.6-9.9) | 3.8 (2.5-5.8) | 5.4 (3.2-9.1) | 8.4 (5-14.2) | 4.4 (2.7-7) | 3 (2-4.5) | 3.8 (2.4-6) | 3.6 (2.4-5.5) | 3.5 (2.3-5.4) |
| Quintana Roo | 2.5 (1.4-4.6) | 4.3 (2.3-8.2) | 4.3 (2.4-7.8) | 2.8 (1.6-4.9) | 2.5 (1.4-4.4) | 4.6 (2.6-8.1) | 2.1 (1.2-3.5) | 3.6 (2-6.6) | 4.8 (2.6-8.7) | 3 (1.7-5.1) | 2.2 (1.4-3.6) | 3.5 (2.1-5.7) | 3.6 (2.3-5.6) | 3.6 (2.2-5.6) |
| San Luis Potosi | 6 (3.9-9.3) | 8.4 (5-14.2) | 7.1 (4.3-11.5) | 7 (4.6-10.7) | 7.9 (5.3-11.9) | 9 (5.7-14.5) | 5.6 (3.8-8.2) | 12.1 (7.5-19.4) | 11.2 (6.8-18.5) | 8.3 (5.4-12.7) | 6 (4.2-8.6) | 8.8 (5.8-13.1) | 6.4 (4.4-9.4) | 8 (5.5-11.7) |
| Sinaloa | 6.2 (4-9.6) | 6.7 (4-11.5) | 6.8 (4.2-11.1) | 5.1 (3.3-8) | 6.1 (4-9.1) | 7.7 (4.8-12.4) | 4.5 (3-6.6) | 6.4 (3.9-10.4) | 9.5 (5.7-15.7) | 5.7 (3.7-8.8) | 3.8 (2.6-5.6) | 5.2 (3.4-7.9) | 4.8 (3.3-7) | 4 (2.7-6) |
| Sonora | 4.2 (2.7-6.7) | 8 (4.7-13.6) | 6.1 (3.7-10) | 5.8 (3.7-8.9) | 4.2 (2.7-6.5) | 6.2 (3.8-10.1) | 3.5 (2.4-5.3) | 4.9 (3-8.2) | 6.7 (4-11.2) | 5.6 (3.6-8.6) | 3.9 (2.7-5.7) | 4.9 (3.2-7.4) | 4.2 (2.9-6.2) | 5.4 (3.7-8) |
| Tabasco | 5.2 (3.3-8.2) | 8.9 (5.3-15.2) | 8.4 (5.2-13.8) | 5.8 (3.8-9.1) | 5.8 (3.8-8.8) | 7.4 (4.6-12) | 5.4 (3.7-8) | 8.6 (5.3-14) | 11.3 (6.8-18.7) | 7.4 (4.8-11.5) | 5 (3.5-7.3) | 7.1 (4.7-10.8) | 6.1 (4.2-9) | 7.7 (5.2-11.3) |
| Tamaulipas | 6.8 (4.4-10.5) | 11.4 (6.8-19.1) | 10.6 (6.6-17) | 7.2 (4.7-11) | 6.6 (4.4-9.9) | 8.6 (5.4-13.7) | 6.5 (4.5-9.4) | 9.5 (5.9-15.2) | 12.4 (7.6-20.3) | 8.3 (5.4-12.5) | 7.2 (5-10.2) | 8.4 (5.6-12.5) | 6.6 (4.6-9.6) | 6.7 (4.6-9.8) |
| Tlaxcala | 3.3 (1.9-5.8) | 4.5 (2.4-8.4) | 5.9 (3.4-10.3) | 5.1 (3.1-8.4) | 3.5 (2.1-5.9) | 3.3 (1.8-6) | 4.5 (2.9-7) | 6.1 (3.5-10.6) | 6 (3.3-10.7) | 5.4 (3.3-8.8) | 3.5 (2.2-5.4) | 3.5 (2.1-5.8) | 3.6 (2.2-5.6) | 4.9 (3.1-7.7) |
| Veracruz | 8.4 (5.6-12.6) | 13.3 (8.1-21.8) | 12.6 (8-19.8) | 9.7 (6.5-14.5) | 10.1 (6.9-14.9) | 13.5 (8.6-21) | 8.3 (5.8-11.7) | 13.6 (8.6-21.5) | 16.3 (10.1-26.5) | 12.1 (8.1-18) | 8.4 (6-11.7) | 11.5 (7.8-16.9) | 9.3 (6.6-13.2) | 10.9 (7.6-15.6) |
| Yucatan | 9 (5.8-14) | 12.5 (7.4-21.2) | 10.8 (6.7-17.5) | 9.4 (6.2-14.5) | 8.7 (5.8-13.2) | 10.6 (6.6-17) | 6.2 (4.2-9.1) | 12.8 (7.9-20.7) | 13.1 (7.9-21.7) | 9.4 (6.1-14.4) | 6.2 (4.3-9) | 10.7 (7.1-16.1) | 8.3 (5.7-12.1) | 10.6 (7.3-15.5) |
| Zacatecas | 4.7 (2.9-7.5) | 8.7 (5-15.1) | 7.8 (4.7-13) | 5.7 (3.6-9) | 5.8 (3.7-9.1) | 6.5 (3.9-10.8) | 4.1 (2.7-6.3) | 6.2 (3.7-10.5) | 8.2 (4.8-14.1) | 5.2 (3.3-8.4) | 4.2 (2.8-6.3) | 4.9 (3.1-7.8) | 3.9 (2.5-6) | 6.1 (4.1-9.3) |
Colima was taken as a reference value of Poisson regression.
Source: Analysis by author from data taken from: the mortality database of the National Institute of Statistic and Geography and National Population Council: population estimates for the period 1990-2010 and population projections for the horizon 2010-2030.
Discussion
In Mexico mortality rates from LC have increased in the past 3 decades 16. In the years 2000-2013, this study identified that the crude death rate from LC increased from 4.2 to 4.9 (percent change of 16.6%) (Figure 1). Similar results have been observed in other studies. The mortality rates from LC for men, reported in Mexico in the periods 1985-1989 and 2000-2005 were 1.44 and 1.95, and for women were 1.29 and 1.90, respectively16. Gómez-Dantés H, et al, reported in 1990, 2,946 deaths from LC and in 2013, 6,594 deaths for this cancer7.
The increase of LC in Mexico could be related mainly to the increase in the prevalence of HBV and HCV, liver cirrhosis from alcohol and fatty liver no associated with alcoholism (associated with obesity)17 and, in the case of the secondary LC could be due to increased incidence of breast cancer18 and colorectal cancer19.
Other countries have also had an increase in mortality rates from LC as the United States of America, Egypt, Japan, Oceania and Europe; and in part, is due to the spread of HCV infection and transfusion of contaminated blood20.
In Mexico in the study period hepatocellular carcinoma was the second leading cause of death from LC with 18,438 deaths (26.5%) after malignant neoplasm of liver unspecified as primary or secondary with 44,192 deaths (63.4%) (Table 2). There are difficulties in distinguishing between primary and secondary LC, which makes complex the epidemiology of this neoplasm20. In this study, without considering the records of malignant neoplasm of liver, not specified as primary or secondary, liver cell carcinoma occurred in 72% of individuals who died of LC (Table 2), these results are similar to those reported in international literature, since it has been seen that between 70% and 90% of PLC are caused by hepatocellular cancer2.
In the study period were registered 44,192 deaths (63.4%) due to malignant neoplasm of liver, not specified as primary or secondary (Table 2). It has been identified that tumors metastatic to the liver are more common than primary tumors. The most common sites of primary tumor are breast, lung, and colorectal cancer.21
In the study population, mortality from LC was increased with age. The highest mortality was identified in the group of 70-74 years old with 10,805 deaths (15.5%) (Figure 2). Cancer is generally a disease of old age22. It has been seen that chronic HCV infection is associated with an increase of hepatocellular carcinoma and its prevalence is relatively high in all age groups, and increases steadily with age23,24.
In individuals with no schooling or incomplete elementary school the RR of dying from LC increased (8.61, 95% CI 8.35-8.89), while individuals with senior in high school or equivalent the RR decreased (0.74, 95% CI 0.71-0.77) (Table 3). The educational attainment is an indicator of health because it has been seen that people with higher education have better possibilities to be employed and to have higher incomes therefore to be prosperous, which directly affects their health25. In Mexico, the lack of education has contributed to the prevalence of social inequality and poverty26. A high level of education is related to the low mortality and a better health of the population27. In Mexico, persons without education or with a low level of it, are usually found in socially, geographically and economically marginalized populations. Individuals of these populations have a higher possibility of dying from preventable cancers like LC. Persons with LC often have underling liver diseases that could be prevented, like liver disease secondary to alcohol (44%), HCV infection (26%), and cirrhosis liver (42%). These diseases often occur in areas of low socioeconomic level where the majority of the people have no schooling28,17.
In other countries, similar results have been found, in the United States, patients with lower educational level (high school) had a higher risk of dying from LC (RR 1.90, 1.22-2.95) than those with higher levels of education (post-graduate)29.
Chihuahua had the highest mortality and risk of dying from LC (Table 4 and 6). In Mexico has been reported that the northwestern region (comprising the states of Baja California, Sonora and Chihuahua) has the highest consumption of illegal drugs. Ciudad Juarez, Chihuahua has the highest increment of use of illegal drug in that region over the past 2 decades. In this state has also increased the intravenous drugs use like cocaine30. Possibly the increase of intravenous drug use is one of the factors contributing to the spread of HBV and HCV, and this increases the prevalence of liver cirrhosis, and therefore a higher mortality rate from LC in Ciudad Juarez, Chihuahua28,31.
The LC has multiple risk factors and epidemiological information of the factors associated with this cancer is very scarce in Mexico. However, today the most important actions to prevent the LC are targeted to control: infection with HBV and HCV, contamination of food by aflatoxin and consumption of alcohol and tobacco as additional preventive measures32.
Conclusions
In the study period, the crude death rate from LC per 100,000 individuals increased from 4.2 to 4.9 (percent change of 16.6%) and died for this cancer 32,734 men (47%) and 36,949 women (53%), with a sex ratio male:female of 0.88:1.0. The malignant neoplasm of liver, not specified as primary or secondary was the cancer most often occurred in patients who had LC with 44,192 deaths, and secondly, the liver cell carcinoma with 18,438 deaths. In individuals with no schooling or with incomplete elementary school the RR of dying from LC was the highest (RR 8.61, 95% CI 8.35-8.89), while individuals with senior in high school or equivalent the RR decreased (RR 0.74, 95% CI 0.71-0.77). Chihuahua had the highest mortality rate and the highest risk of dying from LC [mortality rate 23, 95% CI 19.1-26.9 (2000) and 19.1, 95% CI 15.8-22.3 (2013)] and [RR 30.3, 95% CI 19.6-46.8 (2000) and RR 22.3, 95% CI 15.1-33 (2013)]. Region 2 had the highest mortality rate [5.2, 95% CI 4.9-5.5 (2000) and 7.8, 95% CI 7.4-8.1 (2013)].

