











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
The double-orifice mitral valve (DOMV) is a rare congenital disease first described in 1876 by Greenfield1,2 DOMV has been associated with atrioventricular septal defects, partial or complete atrioventricular canal malformations, aortic coarctation, tetralogy of Fallot, atrial or ventricular septal defect, Ebstein’s anomaly, and patent ductus arteriosus. We present this case to add relevant evidence to the use of multiple imaging modalities for congenital heart diseases, particularly for complex valvular heart disease.
Case presentation
A 29-year-old woman with a 5-year history of hypertension who presented without symptoms since diagnosis. During the control and physical examination, a systolic murmur was found in the left parasternal border as well as a systolic-diastolic murmur in the interscapular area with decreased femoral pulses; CT angiography revealed a coarctation of the thoracic aorta near the left subclavian artery (Figure 1). Echocardiography was performed using the ACUSON SC2000™ ultrasound system (Siemens, Munich, Germany), which showed a bicuspid aortic valve (Figure 2) with moderate stenosis (maximum velocity of 3.4 m/s, maximum gradient of 31 mmHg) and a double-hole mitral valve with thickened valves, insufficient chordae tendineae and two papillary muscles. The posteromedial muscle was hypoplastic and two cords were inserted into the anterolateral muscle, with a mean gradient of 4 mmHg, a mitral valve area of 1.3 cm2, and a severely insufficient eccentric jet through the posterolateral wall of the atrium left with the Coanda effect. The mitral valve orifices were a small orifice in the middle and a larger lateral orifice, which according to the classification of Baño-Rodrigo, can be classified as type 5 or type 2 and is not associated with defects of the atrioventricular canal3-5 (Figure 3). A CMR was performed to confirm the bicuspid aortic valve and double-hole mitral valve (Figures 4 and 5). The patient underwent surgical mitral valve replacement and was discharged without complications after five days. One month after surgery, the patient was asymptomatic in NYHA class I.
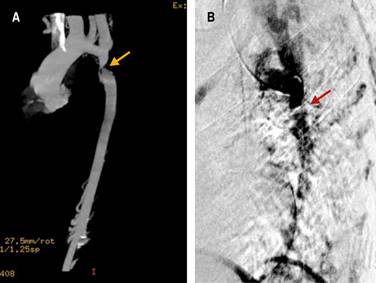
Figure 1: Reconstructed CT aortogram showing localized narrowing of the aorta. A) Reconstruction of the coronal angio-tomography, the projection shows the coarctation site that is 21 mm from the left subclavian artery. B) Digital subtraction angiography showing the thoracic aorta with coarctation.

Figure 2: 2D transesophageal echocardiography at the mild esophageal projection at 57o showing the bicuspid aortic valve.

Figure 3: Real-time 3D transesophageal echocardiography of A atrial face and B ventricular face. It is an eccentric type of double port mitral valve with a larger main port and a smaller accessory port located at the anterolateral commissure.

Figure 4: A) A rendered image of the 3D contrast magnetic resonance angiogram showing the thoracic aorta. B) Cine CMR image of the bicuspid aortic valve in systole (yellow arrow).
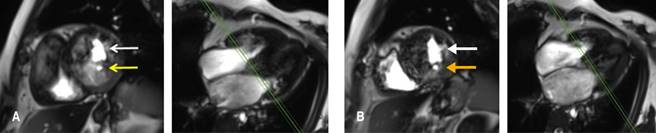
Figure 5: Cardiac magnetic resonance image ( Siemens Verio 3T ). A) Image acquired with the SSFP sequence showing the mitral valve in diastole and the double orifice of the mitral valve (white and yellow arrows). Along the short axis, where the tips are in diastole, the image shows the double mitral orifice, where the posterior orifice is the most minor (yellow arrow) with an area of 0.17 cm2, and a smaller accessory orifice it is located anterolaterally commissure. B) Images of the SSFP sequence along the short axis at the apical level of the double mitral foramen (white and yellow arrows). Parallel green dashed lines indicate the cut-off position to image valve tips to assess the valve area.
Discussion
Aortic coarctation has been reported to be associated with bicuspid aortic valves in 30 to 80% of cases; in the present case, the patient also had a congenital malformation of the mitral valve, which is rare and occurs in only 0.05% of all congenital heart diseases. DOMV has been widely associated with septal defects and with a complete or partial atrioventricular canal in 0.05% of cases.6 In this particular case, in addition to the aortic coarctation and the bicuspid valve, the patient was asymptomatic; This association has been rarely described in the literature, and as far as we know, this is the third case reported to date.
DOMVs can be anatomically classified into central, valvular, and commissural categories according to their structures or conditions; DOMV can also be classified by two-dimensional echocardiography as follows: 1) complete bridge (15% of cases), both orifice openings are circular and visible from the edge of the valve, with normal subvalvular system and papillary muscles; 2) incomplete bridge, missing valve connection and can only be visualized on the edge of the valve; and 3) hole type (most common), typically a minimally sized accessory hole in the posteromedial or anterolateral commissure.7,8 In this particular patient, the VMOV was diagnosed as type 2 according to the Baños-Rodrigo classification, since the accessory orifice (the smallest) is located in the posteromedial commissure.5
Accessory holes are made by different mechanisms that result in DOMV:5
Ring of strings
Subdivision of the muscular crest
Fused papillary muscle
Crossing of strings
Central fibrous subdivision
The bicuspid aortic valve has not been related to DOMV, and although its coexistence has been described in up to 50% of cases, there is no relationship in adults; therefore, this case presents this rare anomaly and associated congenital malformations.
This case exemplifies the importance of the different cardiac imaging techniques since the patient was referred for probable aortic coarctation. The CT aortogram was the initial imaging study performed. Then a transthoracic echocardiogram was performed; because the bicuspid aortic valve and DOMV were found, MR was necessary and useful to determine the timing and definitive surgical treatment.

